
Translate this page into:
Idiopathic chondrolysis of the hip
Address for correspondence: Dr. Shefali Gupta, 1302, Elco Residency, Almeida Park, Bandra West, Mumbai - 400 050, Maharashtra, India. E-mail: guptashefali27@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Gupta S, Choudhary MM. Idiopathic chondrolysis of the hip. J Orthop Allied Sci 2015;3:68-71.
Abstract
Idiopathic chondrolysis is a rare condition characterized by the ultimate loss of femoroacetabular articular cartilage seen in a child with no history of trauma, slipped capital femoral epiphysis, infection, prolonged immobilization, or any other previously described disorder. The diagnosis is often delayed secondary to the insidious onset of symptoms, progressive radiographic findings, and the absence of diagnostic laboratory test. Typical radiographic features include localized osteoporosis, subchondral erosions, femoral head changes, and reduction of the joint space. Later changes include complete loss of the joint space, subchondral cysts, trochanteric and epiphyseal physeal closure, osteophytes, and in severe cases, protrusio acetabuli, ankylosis, and osteoarthritis. Magnetic resonance imaging of the hip demonstrates cartilage loss, joint effusion, marrow edema, femoral and acetabular remodeling, significant regional muscle atrophy, and synovial enhancement. We report a case of Idiopathic chondrolysis of the hip in an 11-year-old Indian girl.
Keywords
Hip
idiopathic chondrolysis
magnetic resonance imaging

Introduction
In the literature, the description of idiopathic chondrolysis of the hip (ICH) in the pediatric age group is rare, being mostly restricted to case reports. ICH most frequently affects female adolescents of Asian or African ethnicity, and is commonly monoarticular (60% affecting right side). Bilateral ICH occurs in 5% of the cases.[1,2] The typical magnetic resonance imaging (MRI) features of our case enabled the diagnosis which was being managed as a case of monoarticular arthritis of the hip.
Case Report
An 11-year-old female child presented to the OPD with complaints of stiffness in her left hip with abnormal gait for 2 months.
There was no history of trauma, constitutional symptoms, or any other joint involvement. The patient had symptoms of pain in the left hip since last one year which was continuous, dull aching and got exaggerated with activity. Pain had now subsided with a significant loss of range of motion.
An initial radiograph done then had revealed a minimal joint space reduction in the left hip. The femoral epiphysis appeared normal in contour and position [Figure 1].

- Anterior-posterior radiograph of the pelvis obtained 2 months after onset of symptoms. Joint space narrowing seen superomedially in the left hip joint. Left femoral epiphysis appears normal in contour and position
MRI done at the same time had revealed a focal geographic area of marrow edema in the central third of femoral epiphysis [Figures 2 and 3]. No depression of subchondral growth plate, erosions or changes in acetabulum were seen. Mild joint effusion was seen. Mild cartilage loss was also seen especially overlying the central femoral head as seen on proton density images [Figure 4a and b].
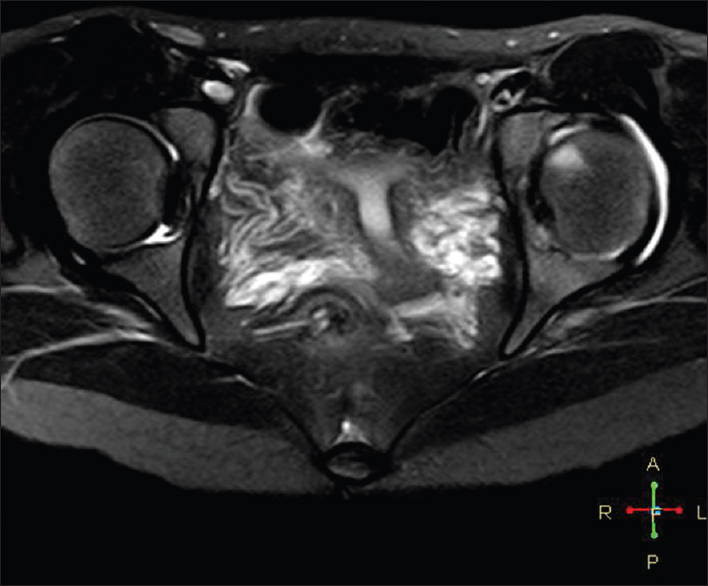
- Noncontrast T2-weighted high-resolution axial image of the pelvis demonstrated a well-defined geographic wedge shaped area of marrow hyperintensity in the left femoral epiphysis. Joint effusion was seen
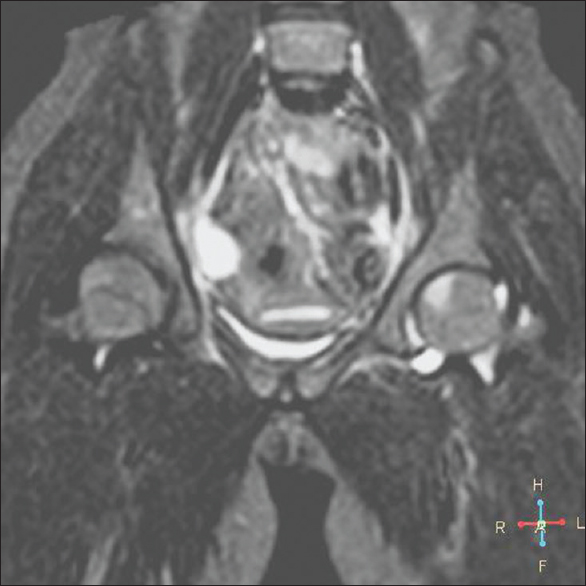
- Coronal short tau inversion recovery images including both hips reveals a T2 hyperintense area in the left femoral epiphysis involving the middle third of epiphysis. Moderate joint effusion also was seen
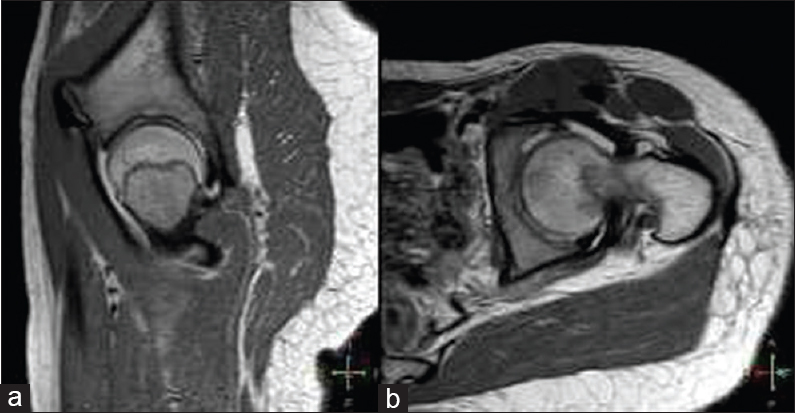
- Proton density weighted sagittal (a) and axial (b) images of the left hip reveal thinning of the articular cartilage overlying the central third of left femoral head
Laboratory values including the complete blood count and white blood cell differential count, erythrocyte sedimentation rate, C-reactive protein, rheumatoid factor, and human leukocyte antigen-B27 were normal. Tuberculin test was negative.
On presentation, the patient had a fixed flexion deformity of 50° with further range of flexion from 50–90°. Abduction, adduction, and rotations were nil. Wasting of left gluteal and thigh muscles were seen.
Fresh radiographs revealed a significant loss in joint space, cortical irregularity of the femoral head, mild protrusio acetabuli, early closure of the epiphyseal plate, and widening of the left femoral head and neck [Figures 5 and 6].

- Anterior-posterior radiograph of the pelvis done 12 months after the symptom onset showed a marked loss of joint space and cortical irregularity of femoral epiphysis. Left acetabular irregularity seen. Protrusio acetabuli present. Early closure of epiphyseal plate seen

- Frog leg lateral view of both hips done 12 months after the onset of symptoms shows a progressive decrease in the joint space of left hip. Irregularity of femoral epiphysis contour seen. Widening of left femoral neck present
Repeat MRI after 12 months of the onset of symptoms revealed extensive loss of articular cartilage with underlying cortical irregularity [Figure 7]. There was a marked increase in the marrow edema now involving anteromedial and posterolateral femoral epiphysis. Subtle left acetabular marrow edema was also present. Joint effusion was present [Figure 8].
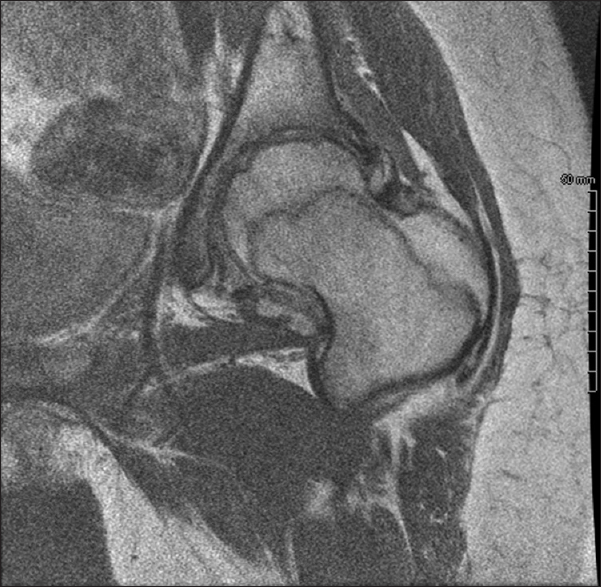
- Proton density coronal image of the left hip demonstrates cortical irregularity of femoral epiphysis and loss of femoroacetabular cartilage

- Coronal short tau inversion recovery image of the pelvis shows extensive T2 hyperintense areas in the left femoral epiphysis with focal areas of overlying cortical irregularity. Mild joint effusion was seen. Atrophy of gluteal muscles seen on the left hip
A retrospective diagnosis of ICH was made. As the patient was unwilling for a surgical intervention, she has been put on left lower limb traction and physiotherapy exercises for improving the range of motion. The patient is under follow up.
Discussion
Chondrolysis in the presence of slipped capital femoral epiphysis was first described by Waldenstrom in 1930. However, it was Jones who described chondrolysis of the hip without a definable cause.[3]
The clinical presentation of the patients with ICH is typically of an insidious onset of pain in the hip, progressive stiffness, and limp.
The cause of ICH remains elusive. Several authors have proposed an immunologic cause for chondrolysis.[4,5,6]
Early radiographic changes, as described by Bleck[7], include regional osteoporosis and blurring of subchondral line with the reduction of the joint space. Late changes include the early closure of capital and trochanteric epiphyses. Severe cases develop fibrous or bony ankylosis. Less severe cases show early changes of osteoarthritis with the development of secondary protrusio acetabuli.
Laor and Crawford[8] described the early MRI features as a geometric or polygonal focal marrow edema pattern centered in the middle third of the affected proximal femoral epiphysis. Associated ill-defined marrow edema in iliac and ischial bone may be seen. This geometric focus could possibly be a watershed type vascular territory where the vascular supply from the medial femoral circumflex artery and the posterior branch of the obturator artery entering along the ligamentum teres meet. Mild cartilage loss was seen suggesting its early onset.
MRI findings of femoral cartilage loss most severe centrally, bone remodeling, and widespread marrow edema in the femoral head, neck, and acetabulum have been reported by Johnson et al.[1] in cases imaged within 9 months of symptom onset.
Differential diagnostic conditions include septic arthritis, toxic synovitis, pauciarticular juvenile rheumatiod arthritis (JRA), slipped capital femoral epiphysis, Perthes disease, and posttraumatic arthritis. Most of these conditions can be excluded on the basis of the clinical presentation, physical findings, radiographic features, and laboratory results.[8] Narrowing of the hip joint space is an important finding that virtually excludes acute synovitis, bacterial and viral arthritis, trauma, and early stages of JRA as the hip joint space is normal or widened in these cases. Monoarticular JRA is predominantly a disease of the knee, ankle, or wrist. The hip joint is very rarely affected, and focal marrow edema has not been described.[8] Slipped capital femoral epiphysis is reliably diagnosed on plain X-rays. The hallmark limited range of motion in all directions of ICH is more extensive than seen in synovitis.
MRI findings of toxic synovitis include joint effusion, synovial thickening and enhancement, and contralateral (asymptomatic) joint effusions. Marrow signal abnormalities are absent.[9] MRI features differentiating septic arthritis from transient synovitis are signal intensity alterations of the bone marrow and signal alterations and contrast enhancement of the soft tissue.
The geographic central and focal marrow abnormality of the femoral epiphysis of early ICH is unlike the diffuse homogeneous or heterogeneous marrow abnormality characteristic of perthes disease.[10] Positive features that aid in the early diagnosis of ICH are the age, sex, and race of the patient presenting with hip pain and with no history of trauma or systemic illness.
Synovial biopsy shows nonspecific inflammation with perivascular infiltrates of lymphocytes, plasma cells, and monocytes but immunofluorescent studies for immune complex deposition are normal. Synovial fluid is unrevealing.[4,6] When left untreated, the natural history of this disease often leads to complete or near-complete ankylosis of the joint.[6] Despite therapeutic options including nonsteroidal anti-inflammatory, physical therapy, traction, and operative interventions such as capsulectomies, hip arthrodesis, and excision arthroplasty, the prognosis is poor.[3]
Conclusion
Early recognition is essential for an accurate prognostication and early therapy to prevent further sequelae.
Financial support and sponsorship
Nil.
Acknowledgment
We wish to acknowledge the constant support and encouragement of the Director of our institute, Prof. PMR, Dr. Rajendra Sharma. We also wish to thank the Assistant Prof., PMR, Dr. Amit Mhambre for his help in Inpatient care.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- Childhood idiopathic chondrolysis of the hip: MRI features. Pediatr Radiol. 2003;33:194-9.
- [CrossRef] [PubMed] [Google Scholar]
- Idiopathic chondrolysis of the hip: A case report and review of the literature. Ann Rheum Dis. 1985;44:268-72.
- [CrossRef] [PubMed] [Google Scholar]
- Idiopathic chondrolysis treated with etanercept. Orthopedics. 2009;32:214..
- [CrossRef] [Google Scholar]
- Idiopathic chondrolysis of the hip: An ultrastructural study of the articular cartilage of the femoral head. Orthopedics. 1986;9:1383-7.
- [CrossRef] [PubMed] [Google Scholar]
- Idiopathic chondrolysis of the hip. Skeletal Radiol. 1996;25:178-82.
- [CrossRef] [PubMed] [Google Scholar]
- Idiopathic chondrolysis of the hip. J Bone Joint Surg Am. 1983;65:1266-75.
- [CrossRef] [Google Scholar]
- Idiopathic chondrolysis of the hip in children: Early MRI findings. AJR Am J Roentgenol. 2009;192:526-31.
- [CrossRef] [PubMed] [Google Scholar]
- MR imaging of transient synovitis: Differentiation from septic arthritis. Pediatr Radiol. 2006;36:1154-8.
- [CrossRef] [PubMed] [Google Scholar]
- Legg-Calvé-Perthes disease: Detection of cartilaginous and synovial change with MR imaging. Radiology. 1988;167:473-6.
- [CrossRef] [PubMed] [Google Scholar]




