
Translate this page into:
Anatomical reconstruction of unstable trochanteric fractures through posterior approach
Address for correspondence: Dr. Partha Saha, Department of Orthopaedics, Nil Ratan Sircar Medical College and Hospital, 138 AJC Bose Road, Kolkata - 700. 014, West Bengal, India. E-mail: partha.orthoatnrs@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Saha P, Ayan S, Bandyopadhyay U, Mukhopadhyay AS, Bhattyacharyya G, Mukhopadhyay K. Anatomical reconstruction of unstable trochanteric fractures through posterior approach. J Orthop Allied Sci 2015;3:55-8.
Abstract
Objective
Unstable intertrochanteric fractures continue to be a challenge for orthopedic surgeons due to the functional limitations it results in the postoperative period. Anatomical reconstruction of the posteromedial fragment becomes difficult through conventional lateral approach, leading to excessive fracture collapse and limping.
Materials and Methods:
A prospective, nonrandomized study was done with 40 patients. They were operated in prone position through posterior approach. Cancellous screws or SS-wires were used to fix the greater or lesser trochanteric fragments and dynamic hip screw (DHS) or dynamic condylar screw (DCS) for the main two fragments. Bone grafts were used to pack cavities at the posterior trochanteric regions.
Results:
Fracture healing occurred earlier compared to conventional lateral approach without excessive fracture collapse in majority of cases (average time to achieve union was 13.8 weeks; range: 10–18 weeks). Good functional recovery was noted with 75% 'Good' or 'Excellent' Harris Hip Scores at 24 weeks.
Conclusion:
Anatomical reconstruction of unstable trochanteric fractures becomes easier through posterior approach with earlier and better functional recovery.
Keywords
Anatomical reconstruction
posterior approach
unstable trochanteric fractures

Introduction
Unstable intertrochanteric fractures of the femur continue to be a challenge for orthopedic surgeons. Despite the high union rates of unstable intertrochanteric fractures,[1] the functional outcomes tend to be disappointing.[2,3] A 60% loss of preoperative independent mobility (or the use of one cane) has been reported in patients with intertrochanteric hip fractures treated with either a gamma nail or a compression hip screw.[2]
Surgical management of unstable trochanteric fractures aims at restoring the pre-fracture functional status of patients as far as ambulatory skills are concerned. A variety of implants of internal fixation have been employed to achieve this goal with variable success.[4]
Our center of attention was comminuted unstable trochanteric fracture (AO classification- TypeA2), where there is loss of the posteromedial buttress, which may or may not be associated with coronal plane fracture of the greater trochanter ('trochanteric burst fractures').[5,6] In absence of anatomical reconstruction of the posteromedial cortex, there is undue fracture collapse (i.e., uncontrolled fracture impaction) resulting in alteration of the femoral neck-offset and the neck-shaft angle along with limb-shortening—leaving the patient with a permanent limp.[7] In addition to this, fractures of the greater trochanter that result in comminution or displacement of the lateral trochanteric wall,[4,8] also requires special attention in order to preserve or restore the normal abductor function of the hip. Traditionally, lateral approach is used to address these unstable trochanteric fractures. But access to the comminuted posteromedial cortex is difficult, at times impossible, through conventional lateral approach; but may become easier through posterior approach to the hip and trochanteric region with patient in prone position.
Thus, the aims of our study were to reconstruct the posteromedial cortex and greater trochanter fracture in anatomical position through posterior approach, first by dealing with this comminution and thus converting the three- or four-part fracture into a two-part fracture and then provide a stable fixation with restoration of neck-shaft angle, which may control excessive fracture impaction, and in turn, provide a limp-free gait.
Materials and Methods
Our study was conducted in the Department of Orthopedics, Nil Ratan Sircar Medical College and Hospital, Kolkata from February 2010 to December 2013 after approval by the Institutional Ethical Committee. It was a prospective, nonrandomized study with a sample size of 40. Patients with comminuted unstable trochanteric fractures with fracture of the posteromedial cortex with/without coronal plane fracture of greater trochanter were included in this study. We had excluded patients with conditions which can adversely affect the postoperative clinical outcome and the rehabilitation process, such as—associated head injury or other major injury, associated fracture of the same/opposite lower limb, pathological fracture, preexisting joint diseases of the same/opposite lower limb affecting its joint mobility, and preexisting neurological problems of the lower limbs (i.e., paraplegia, nerve palsy, etc.). Pre-injury activity level was also kept in mind. All the patients were preoperatively evaluated by X-rays, computed tomography (CT) with three-dimensional (3D) reconstruction and standard investigations for anesthetic fitness. All the patients were informed about the fact that they were included in this study and the data may be used for future publication; and written consents were taken from them. After spinal anesthesia, the patients were placed in traction table in prone position. Skin incision was started 5cm distal and lateral to the posterior superior iliac spine, continued distally and laterally to the posterior part of greater trochanter and then distally along posterior border of trochanter as required.[9]
Subcutaneous tissue and deep fascia were cut in the same line. Gluteus maximus was retracted inferomedially; then lateral intermuscular septum and vastus lateralis were released from their attachment at proximal femur and retracted anteriorly to expose the trochanteric region and posterolateral surface of proximal femur [Figures 1 and 2].

- Gluteus maximus has been retracted inferomedially and lateral intermuscular septum with vastus lateralis has been released from femur and retracted anteriorly. Coronal plane GT fracture has been fixed by a posterior-to-anterior cancellous screw with washer (black arrow); LT fragment by SS-wire (blue arrow), and main two fragments by DHS. GT = Greater trochanter, LT = lesser trochanteric
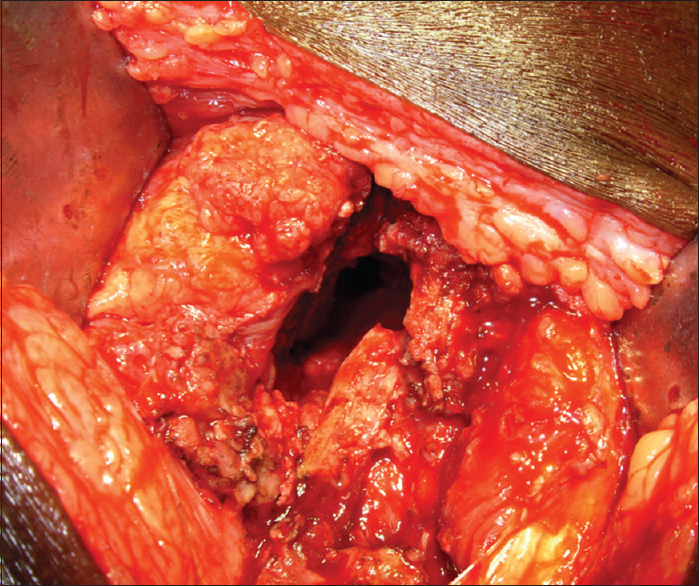
- Cavity at the posterior aspect of trochanteric region as a result of comminution
Under image intensification, the greater or lesser trochanteric fragments were reduced anatomically and fixed using cancellous screws with washer or SS-wires depending on bone quality or fracture configuration [Figure 1]. Then the two main fragments were fixed using dynamic hip screw (DHS) or dynamic condylar screw (DCS) side plates depending on the fracture geometry [Figure 3].
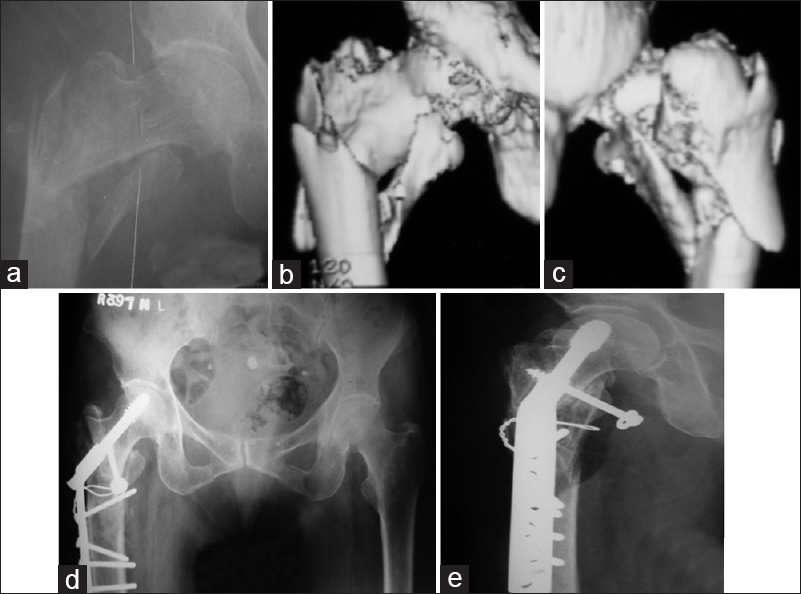
- Pre-and postoperative images of a 60-year-old lady showing four-part unstable trochanteric fracture. (a) Skiagram AP view. (b and c) 3D-CT from anterior and posterior aspects, respectively. (d and e) Postoperative skiagrams at 10 weeks after surgery showing signs of union. 3D-CT = Three-dimensional computed tomography
In these four-part unstable trochanteric fractures, the main comminution lies at the posterior aspect. This results in a cavity or void at the posterior aspect of trochanteric region, which was noted in most of these cases [Figure 2]. The cavity was packed using corticocancellous bone grafts from posterior iliac crest. Fibular strut grafts were used in selected cases where excessive fracture collapse was anticipated (depending on bone quality and fracture comminution). Intraoperative details like operative time, blood loss, number of blood units transfused, etc., were recorded. At around 2 weeks postoperatively, the stitches were removed and active range of movement exercises were allowed. Partial weight bearing was allowed after 6 weeks. Full unprotected weight bearing was allowed only after union was evident.
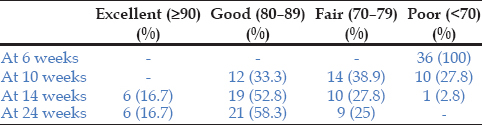
The patients were followed up at 6, 10, 14, 18, and 24 weeks postoperatively, and at 3 months intervals thereafter. Clinical evaluation was done by Harris Hip Score and radiological assessment was done for fracture union [Figure 4], extent of fracture collapse, medial displacement, neck-shaft angle alteration, and implant failure. All baseline and follow-up parameters were described using standard descriptive statistics. While continuous variables were described using means, standard deviations, and ranges; categorical variables were tabulated in percentages.
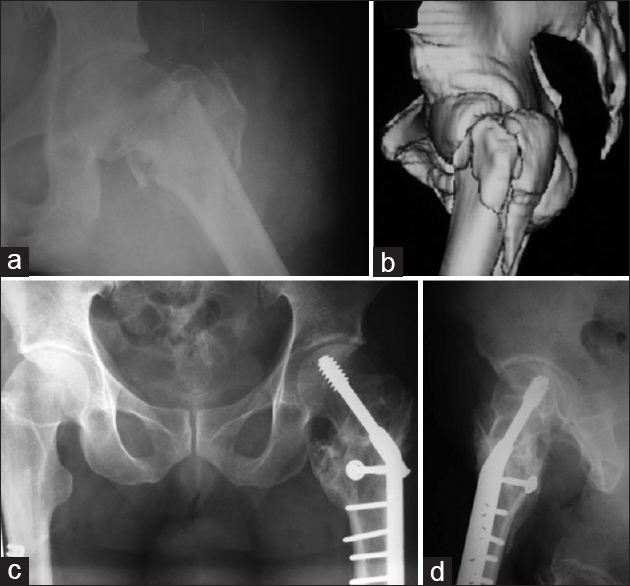
- Pre-and postoperative images of a 37-year-old male patient (a) Skiagram AP view. (b) 3D-CT image showing fracture comminution. (c and d) AP and lateral skiagrams 14 weeks after surgery showing fracture union. AP = Anteroposterior
Results
During result analysis, we excluded the four cases, which were lost to follow-up, thus reducing the effective number of patients to 36. The mean age of our patients were 56 years (range: 32–85 years) with 28 being male. Among them, 14 patients had associated medical problems (hypertension 14 and diabetes 2). The main internal fixation device was DHS in 31 patients and DCS in the rest. The mean operative time was 82.75 min (range: 60–110 min) with a mean intraoperative blood loss of 535 ml (range: 400–800 ml). The average follow-up period of our study was 32.4 months (range: 24–42 months). The fractures united within 14 weeks in 78.9% cases (mean 13.8 weeks; range: 10–18 weeks). One patient had medial displacement with >5° varus collapse. The extent of fracture collapse was measured in percentage of Richard screw length. At 24 weeks, fracture collapse >15% was noted in five patients. Superficial infection was seen in three cases and deep infection in one case. Screw cut out was encountered in one case. However, no complications were noted due to surgery in prone position in traction table.[10] Osteonecrosis of head of femur was not encountered in any case even after a follow-up period of nearly 3 years. The Harris Hip score improved from 'Poor' score in all patients at 6 weeks, to 'Good' or 'Excellent' score in 75% patients at 24 weeks. One 'Poor' score at 14 weeks was due to screw cut out [Table 1].
Discussion
In four-part unstable trochanteric fracture, pull of iliopsoas on lesser trochanter, and gluteus medius on greater trochanter are the main factors leading to displacements. Over the last few decades, it has been established that anatomical reduction of the posteromedial fragment is indispensible in order to achieve stable reduction;[11] and it acts as the main support for the cantilever mechanism of the hip joint and proximal femur to work. Reconstruction of the greater trochanteric and lateral wall fracture is also very important, as it provides a lateral buttress for osteosynthesis and prevents excessive fracture collapse.[4,8]
All the cases were operated by a single surgeon (GB). The average time to achieve union, after modified Dimon and Hughston osteotomy, ranges between 3.5 and 5.5 months.[12] After anatomical reduction it is 18 weeks on an average.[13] However, in our study, it was 13.8 weeks. This early fracture healing in our study was due to packing of cavities at the posterior aspect of the trochanteric region with corticocancellous bone grafts, and anatomical repositioning of the greater and lesser trochanteric fragments which may act like vascularized bone grafts to fasten the fracture healing process.
The incidence of varus angulation of more than 10° after anatomical reduction and fixation with sliding hip screw in literature ranges between 3 and 6%.[14,15] In our study, varus angulation of more than 5° was noted in only one patient. This was due to early weight bearing against advice in the postoperative period.
The average limb length shortening after Dimon and Hughston osteotomy is 1.5 cm (up to 3 cm).[12] But after anatomical reduction, the incidence of more than 2.5 cm of limb length shortening is 3.7%.[14] In our study, the incidence of more than 1.5 cm shortening was 5.6% and it resulted from varus angulation and excessive fracture collapse.
The Richard screw cut out rate through the superolateral part of neck in sliding hip screw fixation after Dimon and Hughston osteotomy is 5.5%[12] and after anatomical reduction it ranges between 4 and 14.9% in different literatures.[10,12,16,17,18] In our study, however, screw cut out was noted in one patient (incidence 2.8%).
Excessive fracture collapse results in shortening of the lever arm of abductor mechanism of hip. This leads to permanent limping and increase in morbidity. In our study, all the five patients who had >15% of fracture collapse scored 'Fair' at 24 weeks. This shows the importance of preventing the excessive fracture collapse in order to improve the final clinical outcome. Therefore, excessive fracture collapse can be controlled by anatomical reconstruction of trochanteric region, packing of posterior comminuted area or cavity (if any) with bone grafts or synthetic bone substitutes, fibular strut graft, and delayed weight bearing. Thus, the advantages of anatomical reconstruction through posterior approach over the conventional lateral approach are: (1) In unstable trochanteric fracture the main comminution lies in the posterior aspect which can be accessed and addressed directly by posterior approach. (2) Direct anatomical reduction and fixation of the posteromedial fragment is possible and easier through posterior approach. (3) It also allows filling of the cavity or void with bone grafts or synthetic bone substitutes. However, the disadvantages of anatomical reconstruction through posterior approach are: Increased operative time and intraoperative blood loss.
Source of Support:
Nil
Conflict of Interest:
None declared.
REFERENCES
- Analysis of six hundred and twenty-two intertrochanteric hip fractures: A retrospective and prospective study. J Bone Joint Surg Am. 1979;61:216-21.
- [CrossRef] [Google Scholar]
- Prospective randomized controlled trial of an intramedullary nail versus dynamic screw and plate of intertrochanteric fracture of the femur. J Orthop Trauma. 2001;15:394-400.
- [CrossRef] [PubMed] [Google Scholar]
- Functional recovery after fracture of the hip: Current concept review. J Bone Joint Surg Am. 1994;76:751-8.
- [CrossRef] [PubMed] [Google Scholar]
- Unstable trochanteric fractures: The role of lateral wall reconstruction. Int Orthop. 2010;34:125-9.
- [CrossRef] [PubMed] [Google Scholar]
- Use of an extramedullary guide pin for fractures of the upper end of the femur. Orthop Clin North Am. 1974;5:525-7.
- [CrossRef] [PubMed] [Google Scholar]
- Symposium on fractures of the hip. Special considerations in management. Orthop Clin North Am. 1974;5:571-83.
- [CrossRef] [PubMed] [Google Scholar]
- Collapse of intertrochanteric hip fractures fixed with sliding screws. Orthop Rev (Suppl 1):30-7.
- [Google Scholar]
- The lateral trochanteric wall: A key element in the reconstruction of unstable pertrochanteric hip fractures. Clin Orthop Relat Res. 2004;425:82-6.
- [CrossRef] [Google Scholar]
- Clinical outcomes of muscle pedicle bone grafting (Meyer's Procedure) in cases of old displaced femur neck fractures: A study of 20 cases. Internet J Orthop Surg 2007:10.
- [CrossRef] [Google Scholar]
- Traction table-related complications in orthopaedic surgery. J Am Acad Orthop Surg. 2010;18:668-75.
- [CrossRef] [PubMed] [Google Scholar]
- Axial loading studies of unstable intertrochanteric fractures of the femur. Clin Orthop Relat Res. 1989;246:156-64.
- [CrossRef] [Google Scholar]
- Unstable intertrochanteric fractures of the hip. J Bone Joint Surg Am. 1967;49:440-50.
- [CrossRef] [Google Scholar]
- Treatment of unstable intertrochanteric fractures with anatomic reduction and compression hip screw fixation. Clin Orthop Relat Res. 1983;175:65-71.
- [CrossRef] [Google Scholar]
- Unstable intertrochanteric fractures of the hip. Treatment with Ender pins compared with a compression hip screw. J Bone Joint Surg Am. 1988;70:1297-303.
- [CrossRef] [Google Scholar]
- Unstable trochanteric fractures. A comparative analysis of four methods of internal fixation. Acta Orthop Scand. 1980;51:949-62.
- [CrossRef] [PubMed] [Google Scholar]
- Unstable intertrochanteric fracture of the femur. A prospective randomised study comparing anatomical reduction and medial displacement osteotomy. J Bone Joint Surg Br. 1993;75:445-7.
- [CrossRef] [PubMed] [Google Scholar]
- Treatment of unstable intertrochanteric fractures of the femur: A prospective trial comparing anatomical reduction and valgus osteotomy. Injury. 1990;21:84-8.
- [CrossRef] [PubMed] [Google Scholar]
- Intertrochanteric femoral fractures. Mechanical failure after internal fixation. J Bone Joint Surg Br. 1990;72:26-31.
- [CrossRef] [PubMed] [Google Scholar]




