
Translate this page into:
A simple technique to correct angular deformity in metacarpal during distraction of osteogenesis
Address for correspondence: Dr. Bakul Arora, Department of Orthopaedics, Father Muller Medical College, Kankanady - 575 002, Mangalore, Karnataka, India. E-mail: bakul_arora@rediffmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Menezes R, Arora B, Acharya P. A simple technique to correct angular deformity in metacarpal during distraction of osteogenesis. J Orthop Allied Sci 2015;3:48-50.
Abstract
Distraction osteogenesis is standard for bone lengthening. The use of Joshi's external stabilizing system (JESS) fixators are common for lengthening of metacarpals. However, being a uniaxial fixator, occurrence of angular deformity is possible. The use of strong dynamic fixators aid in prevention and correction of angular deformities of long bones. We report a simple method to correct angular deformity of metacarpal using JESS fixator, in a 14-year-old girl who presented with congenitally short 3rd metacarpal.
Keywords
Distraction osteogeneis
JESS
metacarpal

Introduction
The correction of deformity is a fundamental part of orthopedic surgery, the desire to elongate a short limb and correct a deformed one is as old as orthopedics itself.[1] However, the first attempt to lengthen a limb was initiated no more than 90 years ago. Following the work of Codivilla,[2] there have been numerous attempts at improving limb lengthening.
The introduction of the concepts of Ilizarov has had a profound effect on understanding and management of deformity. Distraction osteogenesis is widely used for limb lengthening and also for complications of fractures. Currently, it is believed that a delicate distraction rate of no more than 0.25 mm every 6 h is necessary for creating new bone in the distraction gap and acute correction can impair medullary blood supply, which in turn inhibits osteogenesis.[3,4]
The use of JESS mini fixators in hand surgeries, enables the surgeon to counter various challenges posed during the delicate procedures. We report a simple technique to correct angular deformity using JESS fixators.
Case Report
A 14-year-old girl presented to us with a short middle finger of right hand. History revealed that the shortening was noted insidiously by the patient while playing basketball. No previous history of significant trauma. Examination revealed a unilateral shortened middle finger with no rotational or angular deformities. The shortening was about 15 mm compared to the opposite side. Range of movement of the metacarpophalangeal (MCP), proximal interphalangeal (PIP) and distal interphalangeal articulations (DIP) joints of the middle finger were full and pain free. Grip strength was good. No other congenital deformities of limbs or spine were present. Radiograph of the hand revealed shortened 3rd metacarpal. Bone lengthening was offered for cosmesis.
Corticotomy was performed at the neck of the metacarpal through the dorsal approach and the JESS fixator was fixed [Figure 1a]. Gradual distraction was begun after a latency period of 7 days at the rate of 0.25 mm every 6 hours. During the distraction phase, radiographs revealed an angular deformity that was noted in the sagittal plane [Figure 1b]. To correct the angulation during the distraction phase, an additional JESS fixator mini-rod was applied to the construct in the static mode. This negated the angular forces as further distraction was continued for a total of 15 days.

- Post operative radiograph showing the corticotomy at metacarpal neck with JESS mini-fixator in situ (a). As distraction began on the 7th postop day, an angular deformity was noted at the distraction site (b). An additional JESS mini-rod was applied in the static mode which corrected the deformity as distraction continued (c)
During the consolidation phase, the patient was permitted to gradually mobilize her fingers and the radiographs revealed a good regeneration and no angular deformities. [Figure 1c] The fixators were removed after 6 weeks and active finger mobilization began. Subsequent follow-up visits at 3 and 6 months were uneventful. Patient had no residual finger stiffness.
Discussion
A simple lengthening of several centimeters or transportation of a bony fragment along a straight line may be achieved using almost any external fixator. The difficulties arise when a correction has to be carried out three dimensionally. It is important that the limb axes, particularly the joint axes, be identical with the fixator axes, whenever possible. This facilitates three-dimensional simultaneous correction of bone deformities. Clinical cases requiring complex, three-dimensional corrections are not exceptional. Previously, such clinical cases were solved in stages - the angular deformity was solved first, and then the limb was lengthened.[1]
Paley et al.,[5] and Dendrinos et al.,[6] successfully corrected deformity and the inequality of limb lengths using uniaxial monofixators and described the use of dual rods, which adds stability and negates the angular deforming forces while distraction.
Chanchit Sangkaew[4] also recommended the use of dual rod technique during distraction to prevent angular deformity in femur using the AO/ASIF tubular fixators. He named this technique as "Ratchaprasong technique".
Compared with the Ilizarov ring fixator, the unilateral external fixator is simpler to apply and better tolerated by patients.[7,8] The learning curve for implementation of the unilateral fixator is less steep than that encountered with the Ilizarov ring fixator. The JESS minifixator is a unilateral one and also a versatile implant for distraction osteogenesis. It can be applied to the short tubular bones for lengthening and correction of angular deformity without changing the device or need of special accessories.[4]
The authors implemented the principles of the Ratchaprasong technique and combined it with the advantages of JESS minifixators to achieve linear distraction and angular correction during the distraction phase. The addition of an additional rod in the static mode during the distraction phase prevents and corrects the angular deformity during distraction [Figure 2].
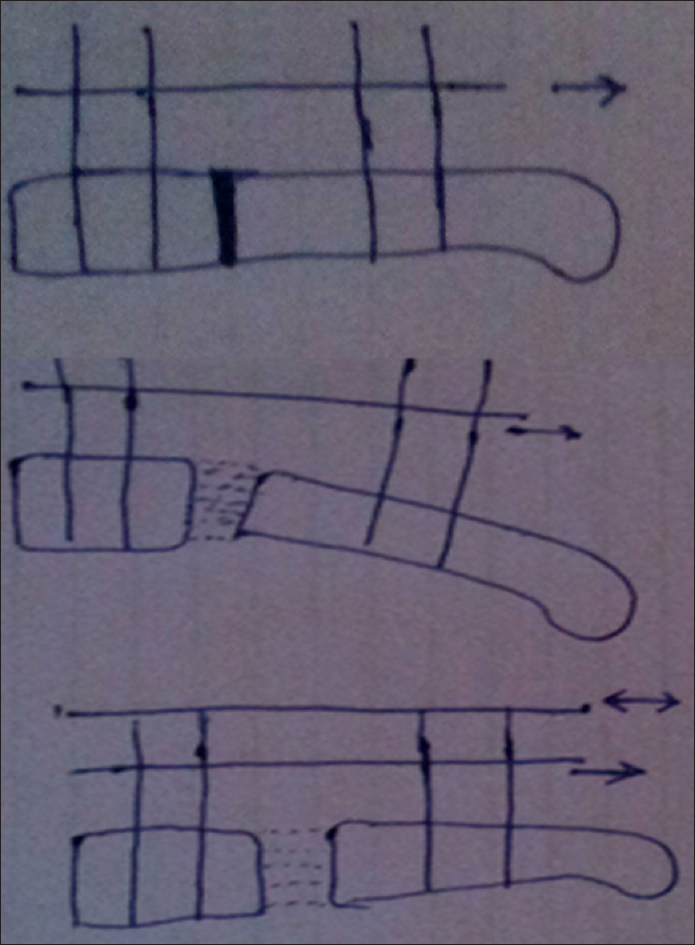
- Illustrated diagram explaining the correction of angular deformity by application of an additional rod in static mode while distraction is continued
Conclusion
The authors recommend the use of dual rod technique using JESS minifixators to prevent and correct angular deformity and achieve linear distraction during the distraction phase of distraction osteogenesis.
Source of Support:
Nil
Conflict of Interest:
None declared.
REFERENCES
- Limb lengthening and three-dimensional deformity corrections. A retrospective clinical study. Arch Orthop Trauma Surg. 1990;109:334-40.
- [CrossRef] [PubMed] [Google Scholar]
- On means of lengthening in the lower limbs, the muscles and tissues which are shortened through deformity. Am J Orthop Surg. 1905;2:353..
- [Google Scholar]
- Clinical application of the tension-stress effect limb lengthening. Clin Orthop Relat Res 1990:8-26.
- [CrossRef] [Google Scholar]
- Distraction osteogenesis for the treatment of post traumatic complications using a conventional external fixator. A novel technique. Injury. 2005;36:185-93.
- [CrossRef] [PubMed] [Google Scholar]
- Ilizarov treatment of tibial nonunion with bone loss. Clin Orthop Relat Res 1989:146-65.
- [Google Scholar]
- Use of the Ilizarov technique for treatment of non-union of the tibia associated with infection. J Bone Joint Surg. 1995;77:835-46.
- [CrossRef] [PubMed] [Google Scholar]
- Correction of complicated extremity deformities by external fixation. Clin Orthop Relat Res 1989:166-76.
- [CrossRef] [Google Scholar]
- Management of nonunion of fractures by distraction correction of angulation and shortening. J Bone Joint Surg. 1996;78:105-9.
- [CrossRef] [Google Scholar]




