
Translate this page into:
Transient osteoporosis of hip
Address for correspondence: Dr. Mahesh M. Choudhary, A-5, Hyderabad Estate, Nepean Sea Road, Opp. Priyadarshani Park, Mumbai - 400 026, Maharashtra, India. E-mail: drmahichoudhary@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Choudhary MM, Ramesh J, Gupta S. Transient osteoporosis of hip. J Orthop Allied Sci 2015;3:44-7.
Abstract
We report a case of transient osteoporosis of the hip (TOH) in a 50-year-old man including the clinical presentation, diagnostic studies, management, and clinical progress. TOH is a rare self-limiting condition that typically affects middle-aged men or, less frequently, women in the third trimester of pregnancy. Affected individuals present clinically with acute hip pain, limping gait, and limited ranges of hip motion. TOH may begin spontaneously or after a minor trauma. Radiographs are typically unremarkable but magnetic resonance (MR) imaging studies yield findings consistent with bone marrow edema. TOH is referred to as regional migratory osteoporosis (RMO) if it travels to other joints or the contralateral hip. TOH often resembles osteonecrosis but the two conditions must be differentiated due to different prognoses and management approaches. The term TOH is often used interchangeably and synonymously with transient bone marrow edema (TBME).
Keywords
Magnetic resonance
transient osteoporosis of hip
regional migratory osteoporosis
transient bone marrow edema syndrome

Introduction
Transient osteoporosis of the hip (TOH) is a rare self-limiting condition that typically affects middle-aged men or, less commonly, women in the third trimester of pregnancy. Exact incidence is not mentioned in literature, but male to female ratio is 3:1. Around 20 cases have been reported in patients of osteogenesis imperfecta. Condition is relatively rare and unique because proper diagnosis leads to improvement without any intervention as in other hip pathologies. These individuals present without a history of major trauma but usually develop an acute onset of hip pain accompanied by decreased ranges of motion, and a limping gait.[1,2,3,4,5,6] Radiographs of TOH are frequently unremarkable, but may display diffuse osteopenia of the femoral head and neck. The affected area appears "warm" on bone scans; however, this test is seldom used due to its low specificity for TOH.[1] Computed tomography (CT) findings include reduced bone density of the affected area and loss of thickness with continuity of vertical primary compressive trabeculae. Magnetic resonance (MR) imaging (MRI) yields findings consistent with bone marrow edema-low signal intensity of bone marrow on T1-weighted sequences and high signal intensity of bone marrow on fluid-sensitive (T2-weighted and fat-suppressed) sequences.[3] The edema affects the subchondral bone of the femoral head and can extend towards the neck and intertrochanteric region. Unlike osteonecrosis, TOH does not result in collapse, fragmentation, or remodelling of the cortical bone of the femoral head nor does it progress to arthritis.
Cases of TOH have been reported with and without the co-existent presence of subchondral stress fractures of the femoral head.[1,2,3,4] The susceptibility to stress fractures may be partly due to diminished bone density secondary to increased osteoclastic activity.[3] There has been debate within the literature whether TOH is a consequence of a stress fracture or vice versa, since not every patient with TOH has subchondral stress fractures.[3,4]
Although the specific risk factors for TOH are poorly understood, it is generally agreed that they differ from the risk factors associated with osteonecrosis.[1,3,4,5,6,7] For example, it is postulated that there may be a relationship between TOH and reflex sympathetic dystrophy, also known as complex regional pain syndrome (CRPS).[3,5,6] The two conditions share similar signs and symptoms of pain, edema, and inflammatory soft tissue changes; however, the hypersensitivity, vasomotor dysfunction, temperature, and skin changes typically observed in CRPS are not characteristic of transient osteoporosis.[3,5] A small retrospective study[6] (n = 17) reported that physicians had a higher incidence of TOH compared to osteonecrosis or transient bone marrow edema syndrome and postulated that this may be due to long hours of standing.
Hip is classically involved, but there are reports of involvement of the knee, ankle, and the foot. TOH may eventually migrate to other hip, a condition referred to as regional migratory osteoporosis (RMO).[5,8] The signs and symptoms of RMO are identical to TOH and both eventually resolve without treatment, suggesting that these are variations of the same or a similar condition.[8]
TOH is also similar to a condition termed transient bone marrow edema (TBME) syndrome. Within the literature, authors may either use the terms interchangeably[3] or choose to differentiate the two conditions. According to some authors,[5,7] TBME syndrome should be reserved for cases where radiographs do not show osteopenic changes of the femoral head and neck, whereas the term TOH is typically reserved for cases where radiographs do demonstrate osteopenia. Aside from this minor distinction the clinical presentation and MR findings of TBME syndrome and TOH are equivalent.[5]
Case Report
A 50-year-old male patient, senior executive by occupation, presented with complaints of pain in the left hip joint with limping since 2 months. Pain was intermittent in variety, radiating through the left thigh up to knee. It started after an episode of heavy exertion during a party organized at his home. Pain was aggravated by weight bearing, walking and there was mild rest pain. Patient did not have any history of trauma, any constitutional symptoms or any other rheumatic complaints in the past. He did have a history of occasional alcohol consumption and smoking.
Examination findings included anterior hip tenderness and terminally restricted internal rotation and flexion. Flexion, Abduction, External Rotation, and Extension (FABER) test was negative and active straight leg raise test SLR were possible but painful. Examination of lumbosacral spine, left knee, and bilateral sacroiliac joints was normal.
Patient was initially investigated with X-rays of pelvis with both hips anteroposterior and frog leg lateral views [Figure 1a and b] and X-rays of lumbosacral spine which was normal. An ultrasonography of the left hip was done which did not reveal any abnormality. Patient was put on a trial of anti-inflammatory drugs and reviewed at 1 week wherein patient did not show any improvement in pain but developed fever; hence, MRI scan of left hip was advised along with base line hematological parameters. MRI revealed features suggestive of transient osteoporosis of the hip (TOH) without evidence of avascular necrosis of the head of femur. His blood parameters including erythrocyte sedimentation rate (ESR), Sr. Alkaline phosphatase, serum creatinine, and serum vitamin D 3 were normal. C-reactive protein (CRP) was elevated to a value of 140.50; hence, a Tc 99 bone scan was done which again documented TOH, but did not rule out infection. Hence, finally, a positron emission tomography (PET) scan was done which significantly ruled out infection. Short tau inversion recovery (STIR) coronal images of the pelvis revealed hyperintense signal in the left femoral head and neck, suggestive of diffuse edema. There was evidence of joint effusion. Femoral head contour was maintained with no evidence of subchondral fracture, no synovitis seen [Figure 2a and b].

- (a and b) X-rays of pelvis with both hips anteroposterior and frog leg lateral view which were normal
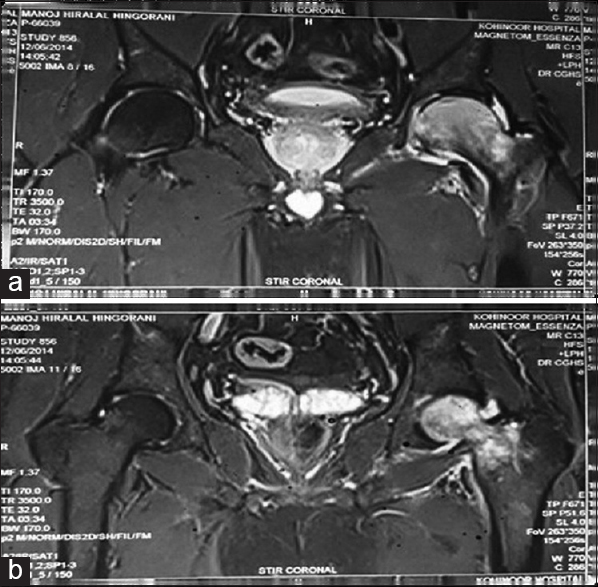
- (a and b) STIR coronal images of the pelvis reveal hyperintense signal in the left femoral head and neck, suggestive of diffuse edema. There is evidence of joint effusion. Femoral head contour is maintained with no evidence of subchondral fracture, no synovitis seen
Coronal T1 weighted image of the pelvis showed a hypointense band convex with the articular margin in the left anterosuperior femoral head suggestive of a subchondral fracture. Surrounding T1 hypointensity seen in left femoral head and neck which appeared hyperintense on STIR images suggestive of diffuse edema [Figure 3a and b].
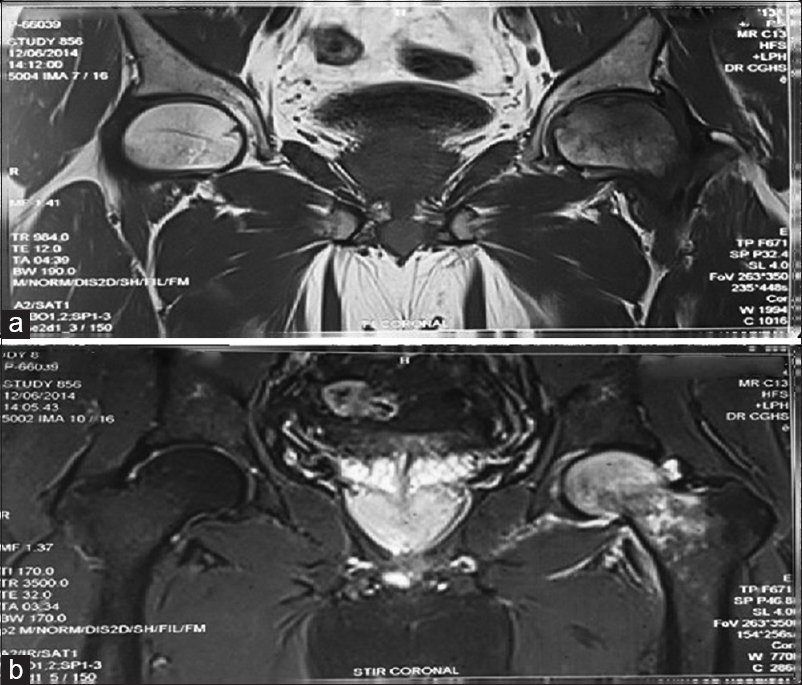
- (a and b) Coronal T1 weighted image of the pelvis shows a hypointense band convex with the articular margin in the left anterosuperior femoral head s/o a subchondral fracture. Surrounding T1 hypointensity seen in left femoral head, neck which appears hyperintense on STIR images s/o diffuse edema
Moreover, 99 Tc bone scan reveals increased radiotracer uptake in the region of left femoral head and neck [Figure 4].
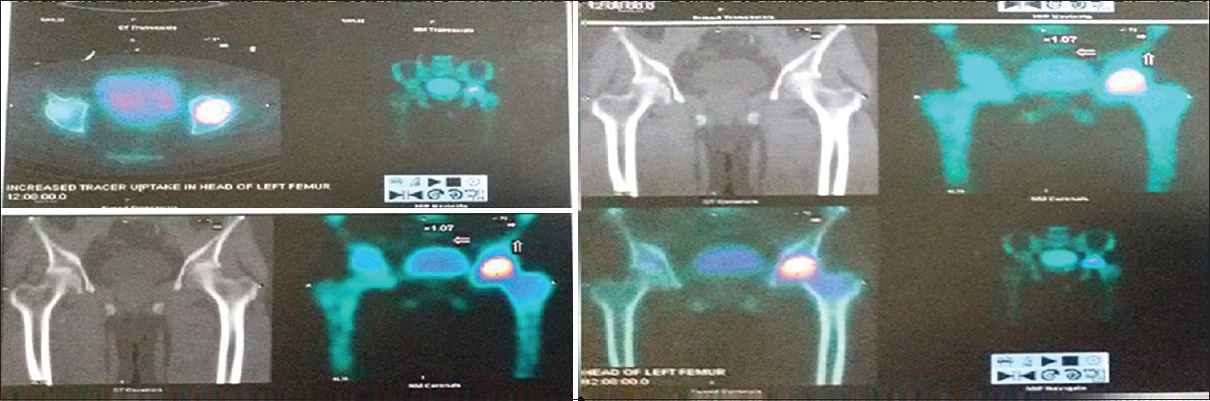
- Bone scan shows increased radiotracer uptake in head and neck of femur on left side
PET CT revealed diffuse increased Fluorodeoxyglucose (FDG) uptake in the head and neck of left femur with standardized uptake value SUV max = 1.6.
Patient was managed with bed rest, anti-inflammatory drugs and calcium and vitamin D supplementation, and was advised to use a walker for activities of daily living (ADLs). He was not given bisphosphonates since he had an episode of dental infection in the recent past. Patient's pain gradually improved over 4 weeks after which he was advised hip range of motion and strengthening exercises. At present with the recent follow-up at 16 weeks, the patient is having negligible pain but limping continues and patient is ambulating with the help of a cane in left hand.
Patients MRI done at approximately 4 months follow up shows complete resolution of bone marrow edema and effusion which proves the diagnosis and management to be appropriate [Figure 5a]-c.
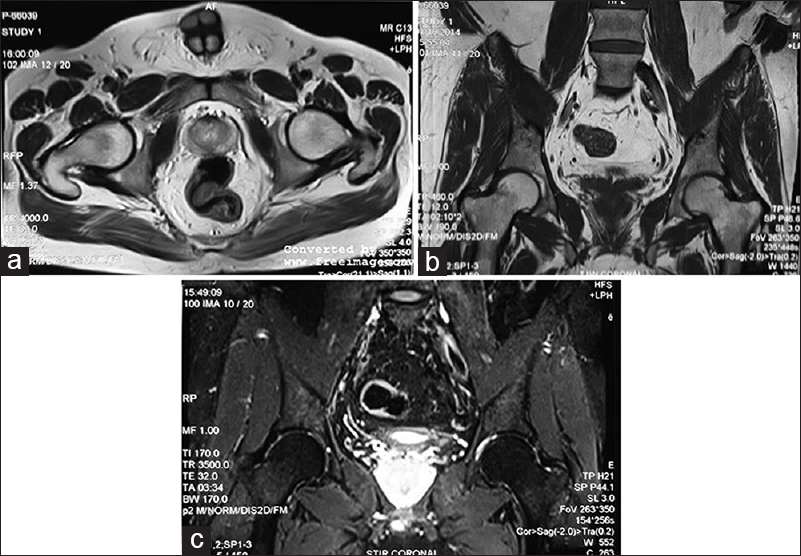
- (a-c) Patients MRI (T1 axial and coronal, STIR coronal) done at 4 month follow up shows complete resolution of bone marrow edema and effusion
Discussion
Transient osteoporosis of hip is a self-limiting condition which predominantly affects males[5] in the age-group of 30 to 50 years.[1] Usually not predisposed by trauma, it presents with unilateral hip pain and limp.[1,3] Cases of TOH in females in third trimester of pregnancy have been reported.[1,2,5,9,10] Unilateral involvement is more common than bilateral one. Initially screening with X-rays may appear normal,[1,3] but MRI scan done for non-resolution of symptoms may reveal typical bone marrow edema without focal lesions. Hip joint effusion seen in this case is also reported with TOH.[1,3,5] Subchondral stress fractures reported in the MRI in this case is a consistent finding in many cases.[3,4]
Complete resolution takes 2-24 months as per various reports.[11] Diwanji recommends follow-up for a period of 24 months.[12] Ergun found direct correlation between the extent of proximal femoral edema and the duration of recovery period. The recovery as per authors gets prolonged if there is a larger subchondral fracture area as seen in the MRI. Migratory recurrence of symptoms occurs within 2 years after pain relief.[13]
Source of Support:
Nil
Conflict of Interest:
None declared.
REFERENCES
- Distinguishing transient osteoporosis of the hip from avascular necrosis. Can J Surg. 2003;46:187-92.
- [Google Scholar]
- CT evidence for subchondral trabecular injury of the femoral head in transient osteoporosis of the hip: A case report. J Korean Med Sci. 2010;25:192-5.
- [CrossRef] [PubMed] [Google Scholar]
- From bone marrow edema to osteonecrosis. New concepts. Reumatol Clin. 2009;5:223-7.
- [CrossRef] [Google Scholar]
- The relationship between MRI findings and duration of symptoms in transient osteoporosis of the hip. Acta Orthop Traumatol Turc. 2008;42:10-5.
- [CrossRef] [Google Scholar]
- MR imaging of bone marrow edema pattern: Transient osteoporosis, transient bone marrow edema syndrome, or osteonecrosis. Radiographics. 1993;13:1001-11.
- [CrossRef] [PubMed] [Google Scholar]
- Male transient hip osteoporosis: Are physicians at a higher risk? Arch Osteoporos. 2009;4:41-5.
- [CrossRef] [PubMed] [Google Scholar]
- Transitory demineralization of the hip in pregnancy. J Bone Joint Surg (Am). 1959;41:1327..
- [CrossRef] [Google Scholar]
- Transient osteoporosis of the hip associated with osteogenesis imperfecta. J Bone Joint Surg Br. 1998;80:54-5.
- [CrossRef] [PubMed] [Google Scholar]
- Transient osteoporosis of the hip in pregnancy: A report of three cases. Acta Orthop Traumatol Turc. 2004;38:229-32.
- [Google Scholar]
- Transient osteoporosis of the hip during pregnancy. J Nippon Med Sch. 2000;67:459-63.
- [CrossRef] [PubMed] [Google Scholar]
- Transient osteoporosis of the hip: MR imaging. Radiology. 1988;167:753-5.
- [CrossRef] [PubMed] [Google Scholar]
- Conservative treatment for transient osteoporosis of the hip in middle-aged women. Singapore Med J. 2008;49:e17-21.
- [Google Scholar]




