
Translate this page into:
Patellar tendon reconstruction with ipsilateral free semi-tendinosus and gracilis autograft for neglected patellar tendon rupture
Address for correspondence: Dr. Appalaraju Sanaboyina, Department of Orthopaedics, Maharajah′s Institute of Medical Sciences, Nellimarla - 535217, Vizianagaram, Andhra Pradesh, India. E-mail: drsaraju@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Sanaboyina A, Rao VM. Patellar tendon reconstruction with ipsilateral free semi-tendinosus and gracilis autograft for neglected patellar tendon rupture. J Orthop Allied Sci 2015;3:40-3.
Abstract
Chronic patellar tendon ruptures are rare. Diagnosis is usually made on clinical background. The ideal method of treatment is a matter of debate. The management of neglected, chronic patellar tendon must address four difficulties: The proximally retracted patella, reconstruction of the patellar tendon, temporary protection of repair, patello-femoral tracking, and active full range of knee movement. By presenting a case of chronic patellar tendon rupture, the advantages of reconstruction with a free semi-tendinosus and gracilis autograft from an early rehabilitation are described.
Keywords
Absent active straight leg raising
free hamstring (semitendinosus and gracilis) graft
modified Insall-Salvati ratio
neglected patellar tendon rupture
patella alta
quadriceps expansion rupture

Introduction
Patellar tendon ruptures are relatively rare injuries caused by forced flexion of knee against an eccentric quadriceps contraction force. These injuries are most common in patients younger than 40 years of age.[1]
Patellar tendon ruptures are also seen in patients with systemic diseases that adversely affect the soft tissues such as rheumatoid arthritis or systemic lupus erthymatosis.[2] Patients with chronic patellar tendon rupture can have significant proximal retraction of patella and sub-optimal tissue for primary repair. These patients benefit from augmentation of patellar tendon repair.[3] Kelikian et al. have described the use of semi-tendinosis for augmentation of patellar tendon rupture. It is a suitable graft because it is strong and native tissue, does not require an additional surgery for removal, and allows for immediate mobilization.[4] Larson and Simonian reported excellent results on a series of four knees in three patients utilizing this technique and an aggressive post op physiotherapy protocol.[5]
Case Report
The patient was a 26-year-old female, who worked as an agricultural laborer. She had ruptured her left patellar tendon 2 years ago when she had an accidental fall while carrying a pot filled with water and landed on her knee in flexion. She had been walking with a hand to knee gait after the fall and had not received any treatment so far; she landed up in our institute 2 years after the injury to get a disability certificate. She did not have any systemic diseases.
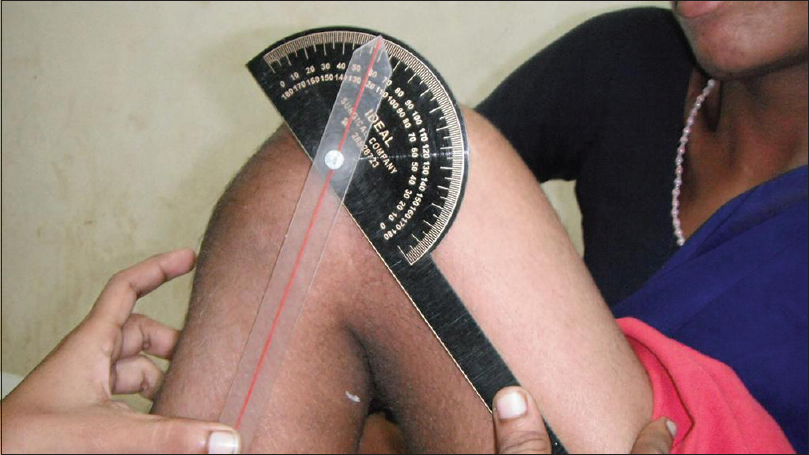
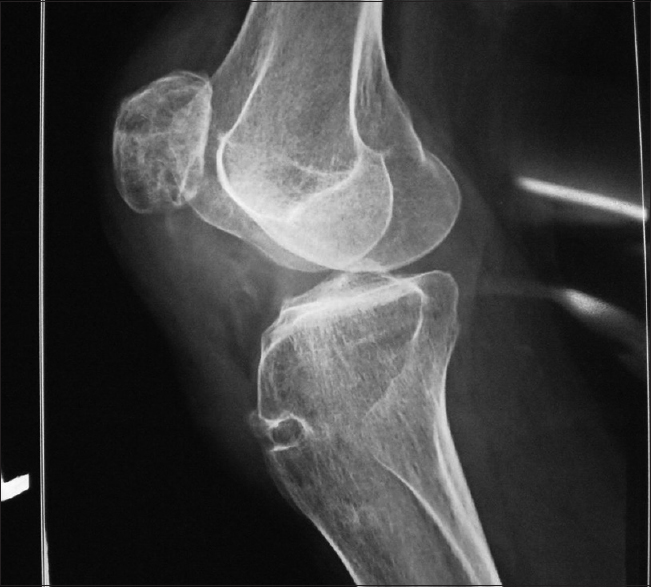
On examination of left knee, no scars were seen, the patella was seen at a higher level and on flexion of knee the shape of distal femoral condyles could be made out [Figure 1]. On contracting the quadriceps by trying to do extension of the knee, the patella was moving upwards. She was using her opposite leg to do a straight leg-raising and there was no active extension of knee possible [http://links.lww.com/JOAAS/A2]. The patella was mobile and could be brought down with no pain. Later X-ray imaging of left knee in 30° showed patella alta but by applying downward pressure, the patella could be brought down to maintain a normal modified Insall-Salvati ratio [Figures 2 and 3]. A surgical intervention was warranted.

- Preop clinical photo showing patella at ahigher level (Large)

- Pre op x-ray showing a high riding patella

- Pre op x-rayof the same knee with patella pushed down by examiner
Patient in supine position with tourniquet under control a median parapatellar incision was made over the left knee. Patella was found to be elevated with rupture of extensor apparatus. Using closed tendon strippers which are used for anterior cruciate ligament reconstruction, semi-tendinosus and gracilis-free tendons are harvested. Single bundle length of 220 mm was obtained with graft dimensions of 220 mm × 6 mm.
Steinman pin is passed through patella to provide traction. Tension band wiring of patella in figure of 8 is done. Extensor apparatus is sutured with ethibond no: 5. Knee range of movement from 0° to 95° is obtained. Patellar tracking is well-maintained. Moreover, 7 mm drill holes are made transversely in patella and tibia over a guidewire using cannulated reamers from anterior cruciate ligament (ACL) reconstruction set. Semi-tendon and gracilis-free graft are passed in a rectangular loop and sutured with ethibond no: 5 [Figure 4]. Wound closed in layers after placing drain. Compression bandage applied. Drain removed on day 2. Passive range of knee movement started on day 4 from 0° to 60°. Full weight-bearing walking with walker started on day 6. At the time of discharge, patient was mobilized full weight-bearing with active straight leg raising possible and active knee range of movement from 0° to 85° [http://links.lww.com/JOAAS/A3].

- Intra op pic showing patella tension band wiring and semitendinosus and gracilis graft
After 6 weeks, removal of Tension band wire done under anesthesia. Intra-operative manipulation of knee was done to get full flexion at knee. Knee closed in layers. From post-operative day 2, patient was started on continuous passive motion. By day 10, she had active straight leg raising positive and knee range of movement from 0° to 120° [Figures 5-7].
- Post op knee flexion upto 120 degrees

- Post op knee extension showing full extent in comparision to opposite knee

- Post op active Straight leg raising the operated knee
After 1 year of follow-up, she had full active knee range of movement from 0° to full flexion [http://links.lww.com/JOAAS/A4] with good patellar tracking and X-ray showing normal location of patella [Figure 8].
- Post op x-ray showing normal location of patella
Discussion
Patellar tendon is a strong and important structure in the extensor mechanism of the knee. Acute patellar tendon ruptures are relatively uncommon and usually occur when forceful quadriceps muscle contraction is resisted by a flexed knee joint.[6] The true incidence of patellar tendon rupture is unknown, but it is the third most common injury to the extensor mechanism, after patellar fracture and quadriceps tendon rupture.[7,8] Diagnosis is made upon clinical examination, inability to extend knee, a palpable defect distal to patella and patella alta. X-ray can be helpful to distinguish patellar tendon ruptures from patellar fractures.[6]
Large trials have never been performed and therefore there are no gold standard protocols for treatment or rehabilitation program. Surgical repair is always indicated unfortunately due to quantitative and qualitative impairment of the tendon fibers, simple reinsertion often is not sufficient or not even possible. Furthermore, a chronic rupture usually is accompanied by abundant scar tissue formation and quadriceps muscle contracture. In this scenario, a patellar tendon augmentation usually is required in order to create a stable and functional extensor mechanism.[6]
Many reconstruction techniques have been proposed: Synthetic material[9,10], autograft using semi-tendinosus alone[11] or together with the gracilis[6] and the contra lateral patellar tendon[8,12] or allograft using Achilles tendon.[13,14,15,16] A contra lateral bone-patellar tendon-bone graft consists of a composite quadriceps tendon, patella, patellar tendon and tibia unit, which allows the extensor mechanism to be reconstructed and the patella to be automatically positioned at the proper height. This technique is most useful when the remaining tendon stump is not adequate or in cases of surgical revision. Despite significant morbidity associated with autografts, allograft techniques have a risk of bacterial or viral infection, neoplasia and especially non-conventional transmissible agent transmission. They should only be considered when the extensor mechanism is extensively damaged and an autograft cannot be used.[17]
The biggest challenge with this surgery is the need to mobilize a non-reducible patella, which was not the case with our patient.
Source of Support:
Nil
Conflict of Interest:
None declared.
REFERENCES
- Patellar tendon repair with hamstring autograft: A cadaveric analysis. Clin Biomech (Bristol, Avon). 2010;25:348-51.
- [CrossRef] [PubMed] [Google Scholar]
- Patellar tendon rupture in systemic lupus erythematosus. J Rheumatol. 1989;16:786-8.
- [Google Scholar]
- Disruptions of the extensor mechanism. Orthop Clin North Am. 1992;23:687-95.
- [CrossRef] [PubMed] [Google Scholar]
- Restoration of the quadriceps function in neglected tear of the patellar tendon. Surg Gynecol Obstet. 1957;104:200-4.
- [Google Scholar]
- Semitendinosus augmentation of acute patellar tendon with immediate mobilization. Am J Sports Med. 1995;23:82-6.
- [CrossRef] [PubMed] [Google Scholar]
- Recurrent patellar tendon rupture: Reconstruction using ipsilateral gracilis and semitendinosus tendon autografts. Injury. 2007;38:320-3.
- [CrossRef] [Google Scholar]
- Traumatic bifocal avulsion of the patellar tendon. Injury. 2005;36:115-7.
- [CrossRef] [Google Scholar]
- Reconstruction of chronic patellar tendon rupture with contralateral BTB autograft: A case report. Knee Surg Sports Traumatol Arthrosc. 2007;15:1445-8.
- [CrossRef] [PubMed] [Google Scholar]
- Concurrent bilateral patellar tendon rupture in a preadolescent athelete: A case report and review of the literature. J Pediatr Orthop B. 2010;19:511-4.
- [CrossRef] [PubMed] [Google Scholar]
- Recurrent bilateral rupture of the patellar tendons: Tendon replacement using polyester connective tissue prosthesis. Injury. 2006;37:379-82.
- [CrossRef] [Google Scholar]
- Augmentation of a patellar tendon repair with an autologous graft. Acta Orthop Belg. 2009;75:417-9.
- [Google Scholar]
- Treatment of old or recurrent ruptures of the patellar ligament by contralateral autograft. Rev Chir Orthop Reparatrice Appar Mot. 1992;78:58-62.
- [Google Scholar]
- Achilles allograft reconstruction of a chronic patellar tendon rupture. Arthroscopy. 1998;14:340-4.
- [CrossRef] [PubMed] [Google Scholar]
- Chronic rupture of a patellar tendon: A technique for reconstruction with Achilles allograft. Arthroscopy. 1996;12:623-6.
- [CrossRef] [PubMed] [Google Scholar]
- Chronic patellar tendon rupture: Surgical reconstruction technique using 2 Achilles tendon allografts. J Knee Surg. 2008;21:130-5.
- [CrossRef] [PubMed] [Google Scholar]
- Two-layer repair of a chronique patellat tendon rupture: A novel technique and literature review. Am J Orthop (Belle Mead NJ). 2010;39:277-82.
- [Google Scholar]
- Chronic patellar tendon rupture reconstruction with a semitendinosus autograft. Orthop Traumatol Surg Res. 2011;97:447-50.
- [CrossRef] [PubMed] [Google Scholar]




