
Reasons for patient′s withdrawal from clinical trials of rheumatoid arthritis in India
Address for correspondence: Dr. Sangeeta Sanjay Dabhade, A-10 Jagaram Complex Dhanori Road, Vishrantwadi, Pune - 411 015, Maharashtra, India. E-mail: sangeetadr99@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Dabhade S, Pandit P, Tiwari S, Pandit D, Chopra A. Reasons for patient's withdrawal from clinical trials of rheumatoid arthritis in India. J Orthop Allied Sci 2015;3:8-11.
Abstract
Introduction:
Rheumatoid arthritis (RA) affects 0.5-1% of population all over the world. As the duration of treatment is more in RA, patient's adherence to treatment is less. Controlling the number of patients lost to follow-up is essential for the successful completion of randomized clinical trials. Also, patient adherence is critical in clinical trial setting as it has impact on validity of clinical data and also it remains an issue of utmost importance to pharmaceutical manufacturers as well as scientific and regulatory community. The studies which show reasons for withdrawal from clinical trials are done for diseases like tuberculosis (TB). None of the study is available to find reasons for withdrawal from clinical trials in RA. Hence, this study is planned.
Aims and Objectives:
Find reasons and effect of age, sex, duration of therapy, and distance from home on withdrawal from clinical trial.
Materials and Methods:
This study is a retrospective observational data analysis. Primary outcome are to find reasons for withdrawal from trial.
Results:
Withdrawal from clinical trial in patients of RA is more in female. In this study, reasons for withdrawal from study are change in location, loss to follow-up, failure of therapy, concomitant illness, patient withdrew consent, and adverse effects is the common reason for withdrawal from clinical trial in both patient and investigator-related reason for withdrawal.
Keywords
Clinical trial
noncompliance
withdrawal

Introduction
Rheumatoid arthritis (RA) affects 0.5-1% of population all over the world. The estimated prevalence of RA in developing countries is variable. The prevalence of RA in India 0.75%.[1] As the duration of treatment is more in RA, patient's adherence to treatment is less.
Controlling the number of patients lost to follow-up is essential for the successful completion of randomized clinical trials.[2] Also patient adherence is critical in clinical trial setting as it has impact on validity of clinical data and also it remains an issue of utmost importance to pharmaceutical manufacturers as well as scientific and regulatory community.[3,4]
Compliance with medical recommendations and the extent to which these are followed as defined is a complex and interesting challenge. Treatment adherence is an approach to maintain or improve health as well as managing symptoms and signs of disease.[5] It is a complex behavioral process influenced by the environment in which patients live, nature of healthcare provider, and place of the healthcare delivery. The rate of default from tuberculosis (TB) treatment occurs frequently.[6] This nonadherence to TB treatment could lead to treatment failure and development of drug resistance.[7]
Psychiatric patients miss about 20% of scheduled appointment for mental health treatment which is almost twice the rate in other medical specialties.[8] A example of non-compliance effect on trial outcome can be observed in the Lescol Intervention Prevention Study (LIPS) retrospective analysis study. In this study a retrospective analysis of the effect of noncompliance on time to first major adverse cardiac event was done. When statistics allowed noncompliance to enter analysis the RR calculated was 32% as against the original RR published which was 22%.[9]
Patient adherence is critical in clinical trial setting as it has impact on validity of clinical trial data. It is an issue of importance as far as scientific and regulatory community and pharmaceutical industry is concerned.[3,4]
A study conducted by Holroy in 2005 demonstrated that 25-50% of participants in clinical trials do not adhere to prescribed drug regimen. This withdrawal of research participants can result in inconsistent or altered study results that lead to misinterpretation of the effectiveness of a drug.[3]
The consequences of withdrawal from therapy in clinical trial are injurious to correct conclusion. The cost of withdrawal in clinical trials can affect trial results to such an extent that they can make or break a candidate drug.[10]
Expenses in research and development in pharmaceutical industry reach up to US $58 billion and approximately 40% of this amount is spent on clinical trials annually. It is estimated that each new marketed drug carries cost of US $1 billion and this figure is constantly growing due to increase in number of patients included in trials.[4]
We searched to find reasons for withdrawal from clinical trials. Very few studies are seen. We could not find any study which shows reasons for withdrawal from clinical trials in Indian setup. The studies which show reasons for withdrawal from clinical trials are done for diseases like TB and psychiatric illnesses. None of the study is available to find reasons for withdrawal from clinical trials in RA. With this background we planned a study to find the reasons for withdrawal from clinical trials.
Aims and objectives
To find reasons for withdrawal of patients from clinical trial
To find effect of age, sex, duration of therapy, and distance from home on patient withdrawal from clinical trial.
Materials and Methods
This study is a retrospective observational data analysis. Population under this study comprises all patients who were enrolled in various clinical trials of rheumatic disease attending Center for Rheumatic Disease Pune in (CRDP) between January 2012 and June 2013. Record of total 1,313 patients in 10 different clinical trials is included in this study. Patients withdrew from the study due to no disease activity. Therefore only 1299 patient's records eligible for analysis.
Primary outcome measures are to find reasons for withdrawal from trial. Withdrawal from trial was defined as patient who at any time after starting treatment had not collected the drug for 1 month or more. Case record forms (CRFs) of all 1299 patients were obtained. The data was analyzed for the demographic characteristics like age, sex, and distance from home and education status. Data was also analyzed to find out reasons for not continuing the trial. The reasons were collected from the patients when they attended the CRDP ≥ 1 month after withdrawal from the study.
Results
More male patients (660) were enrolled as compared to female patients (639). Among the various co morbidities the top three frequently noted were obesity (57%), hypertension (40%) and diabetes mellitus (37%). Educational status did have certain variations as 78% patients enrolled had primary education where as patients with more than primary education were 27%and 18% with higher secondary and graduation respectively [Table 1].

The following Figure 1 shows various reasons for withdrawal from the clinical trial.
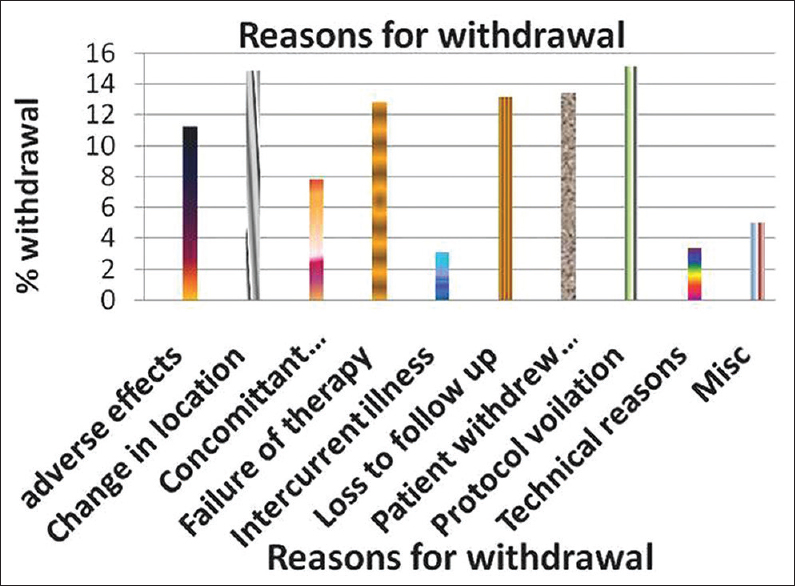
- Shows reasons for withdrawal of patients from clinical trial in rheumatoid arthritis (RA)
The withdrawal of female patients was slight higher than male patients (P < 0.05),
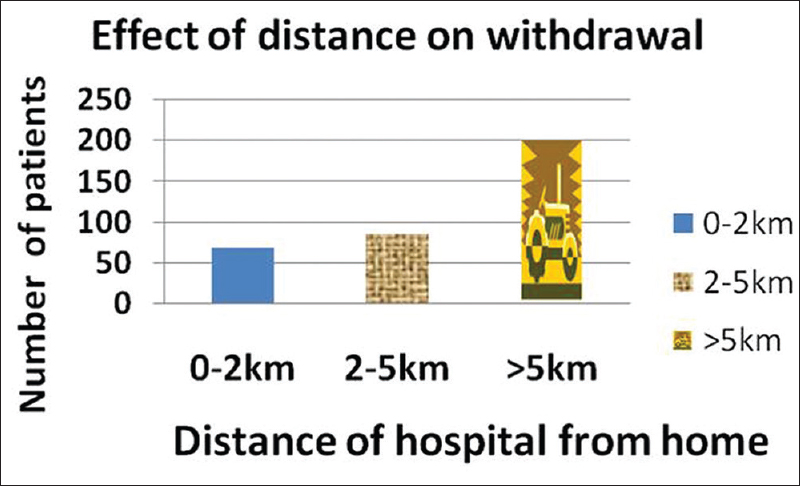
Patients residing at distance of >5 km from trial center did significantly have greater withdrawal rate (P < 0.001) Figure 2 and Table 2. In this study, the commonest reason related to withdrawal from study is change in location (53, 15%). In this study, common reasons related to withdrawal from study are change in location (53, 15%), loss to follow-up (47, 13%), failure of therapy (47, 13%) These may be because of as the distance from the center increases because of change in location this may lead to loss to follow-up which may lead to failure of therapy.
- Shows effect of distance on withdrawal from clinical trial in RA patients

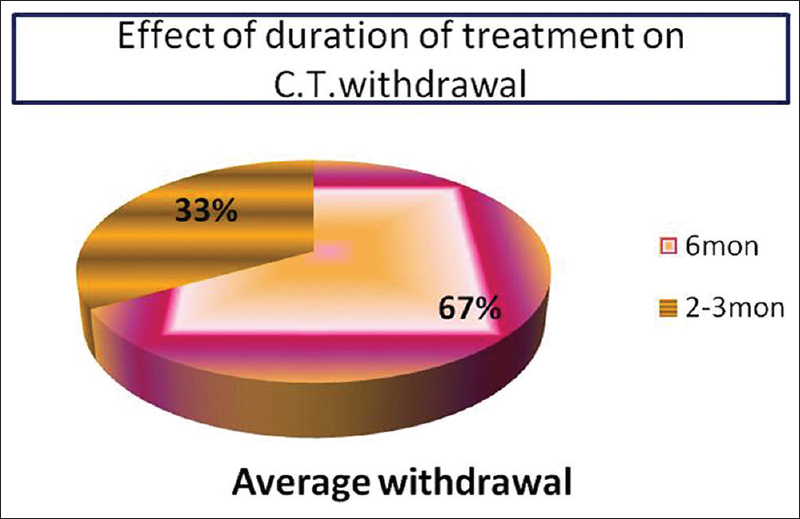
Duration of treatment also had an impact on withdrawal. Study duration of 2-3 month had only 23 withdrawals but it was higher if study duration was 6 month (45 withdrawals) Figure 3 and Table 2.
- Shows effect of duration of treatment on withdrawal of patients from clinical trials of RA
Discussion
Results of this study show that withdrawal from clinical trial in patients of RA is seen significantly more in female than male patients. Surprisingly, it has been seen that enrolment of female patients in this study is less as compared to male patient despite of having more incidence of RA in female.[11]
This may be because of patriarchal system in India where women are given less importance or because of women themselves do not give importance to their health. The result of this study is supported by Genevieve Frank[12] which mentions that women distrust medical research and thus participation in trials is more limited.
In this study distance of hospital or clinical trial center and duration of trial also significantly affected the treatment adherence, this is may be because it does hamper patient's economy as travelling expenses and his/her daily wages.
Several studies suggested that withdrawal from trial is less during 1st month and more withdrawal is seen over the time.[5] Though statistics is not applied to enrolment of patients depending on their education, it has been seen that patient having qualification lesser than primary education have more enrolment. This is because people involved in the trial may be poor and drugs available free of cost in clinical trial. In sub-Saharan Africa, several social factors such as lack of social support; stigma related to disease, and other factors like old age, low education, financial problem, ignorance on need for treatment were related to clinical trial withdrawal.[6]
Withdrawal from clinical trial depends on many factors like modifying lifestyle, behaviors recommended (e.g., smoking cessation), complexity of regimen, and ease with which a patient can incorporate those recommendation into his/her daily routine. Withdrawal from clinical trial also varies according to incentive verses therapeutic intent or goal and ability to pay for care.[5] From decades it has been known that compliance with lifestyle and behavior and drug regimen has been overestimated by both patients and providers.[5]
In chronic disease like RA and TB, patients opt to use herbal medication instead of recommended drugs and this becomes risk factor for withdrawing from clinical trial.[6]
In our study apart from effect of various demographic factors on withdrawal from clinical trials, we found that there are various reasons for withdrawal from clinical trials. In this study, reasons related to withdrawal from study are change in location (53, 15%), loss to follow-up (47, 13%), failure of therapy (47, 13%), concomitant illness (39, 10%), patient withdrew consent (48, 13%), and investigator-related factors were protocol violation (54, 15%) and technical reasons (12, 3%). Adverse effect (40, 11%) is the common reason for withdrawal from clinical trial in both patient- and investigator related reason for withdrawal [Figure 1]. Findings of this study are concomitant to that by Suhadev et al.[7]
Change in location and loss to follow-up contribute major chunk for reasons for withdrawal from clinical trial. This may be because of poor access to public transport, staying far from hospital, or unable to afford transportation expenses and no relative able to send them to hospital.[7,13] As most of the patients with RA are debilitated, disfigured and crippled because of disease, they would require special transport facility.
While searching references to find reasons for withdrawal from clinical trial we found certain pharmaceutical factors. It has been seen that packaging can play an important role in addressing and mitigating a variety of emotional and functional barriers that patients experience during clinical trials. While traditional pharmaceutical packaging-standard bottles and amber vials-do not provide any support for patient in following their treatment regimen, a combined blister and unit dose packaging, clear labeling, child resistant, and senior friendly packaging provide a variety of benefits that encourage prescription compliance and ease of access for patients which adhere patient in the clinical trials.[3,10]
Regarding effect of withdrawing patients due to any reason, ICH E6 guidance for industry mentions that validity of clinical study would also be compromised by the exclusion of data collected during study. There is particular concern with a study's reliability when subjects withdraw their data in nonrandom way because they are unhappy with their experience, either because they failed to obtain a desired effect or suffered an adverse event. Loss of these subject's data could greatly distort effectiveness results and could hide important safety information (e.g. toxicity) of poorly tolerated treatment.
Finally, removal of data due to withdrawal of patient due to any reason would compromise Food and Drug Administration's (FDA's) ability to perform its mission, to protect public health and safety by ensuring the safety and effectiveness of regulated products.[13]
Looking at effect withdrawal on the clinical trials in general, some intervention and motivational strategies should be made to decrease patient withdrawal from clinical trial like providing more convenient care, educate patients, and sending reminder to patients.
Conclusion
Looking towards these trial results there are various reasons for withdrawal from clinical trials. Few of them highlighted in this study. Therefore to conclude, probably enrolling patient's residence within 5km radius of the trial or providing transportation if feasible will be more helpful in decreasing withdrawals in an Indian scenario. An emphasis to plan shorter duration trial keeping in mind the disease pathophysiology as well. The most important observation is gender variation in withdrawals. Special considerations like allowing fewer visits to female patients. Even a special consulting day for female patients which will decrease the frequency of visits may prove helpful to decrease the withdrawal rates from trials. In this trial change in location, loss to follow-up, failure of therapy, concomitant illness also remained as causes of withdrawal from trial.
Source of Support:
Nil
Acknowledgement
Authors would like to acknowledge CRDP (Center for Rheumatic Disease Pune) for providing data for this study.
Conflict of Interest:
None declared.
REFERENCES
- Epidemiology of Rheumatoid Arthritis in a tertiary care unit, Karachi, Pakistan. J Pak Med Assoc. 2011;61:123-6.
- [Google Scholar]
- Factors associated with compliance and non-compliance by physicians in large scale randomised clinical trials. Trials. 2006;7:26. Available from: http://www.trialsjournal.com/content/7/26 (accessed )
- [CrossRef] [PubMed] [Google Scholar]
- The solution to more effective clinical trials: Adherence packaging. Eye for pharma.com 2008 June 5 (accessed )
- [Google Scholar]
- Manager Clinical Trial Solution, Bang and Olufsen Medicom a/s Compliance to drug treatment in clinical trials. business briefing, Technology and services Pharma- tech. 2004 (accessed )
- [Google Scholar]
- The multilevel compliance challenge: Recommendations for a call to a action. A statement for healthcare professional. Circulation. 1997;95:1085-90.
- [CrossRef] [PubMed] [Google Scholar]
- Factors associated with default from treatment among tuberculosis patients in Nairobi province, Kenya: A case control study. BMC Public Health. 2011;11:696..
- [CrossRef] [PubMed] [Google Scholar]
- A retrospective study of non-compliant patients in controlled clinical trials of short course chemotherapy. Ind J Tub. 1995;42:221..
- [Google Scholar]
- Why don′t patients attend their appointments? Maintaining engagement with psychiatric services. Adv Psychiatr Treat. 2007;13:423-34.
- [CrossRef] [Google Scholar]
- A retrospective analysis of the effect of noncompliance on time to first major adverse cardiac events in LIPS. Clin Ther. 2003;25:2431-47.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of pill organizers and blister packs on adherence in two vitamin supplementation trials. Am J Epidemiol. 2000;152:780-7.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiological aspects of rheumatoid arthritis: The sex ratio. Ann N Y Acad Sci. 2006;1069:212-22.
- [CrossRef] [PubMed] [Google Scholar]
- Current Challenges In Clinical Trial Patient Recruitment And Enrollment. Clinical Research Associate. ICON SoCRA SOURCE 2004 February:30-8.
- [Google Scholar]
- Guidance for sponsors clinical investigators and IRBs data retention when subject withdraw from FDA-regulated clinical trials. 2008. U.S. department of health and human services FDA, office of the commissioner good clinical practice program. Available from: http://www.fda.gov/oc/gcp/draft.html (accessed )
- [Google Scholar]




