
Translate this page into:
Apophyses and physeal equivalents in the pediatric pelvis
Address for correspondence: Mr. Vineet Tyagi, Department of Orthopaedic Surgery, New York University Langone Medical Center, 550 First Avenue, New York - 10016, USA. E-mail: vineet.tyagi@med.nyu.edu
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Tyagi V, Milla S. Apophyses and physeal equivalents in the pediatric pelvis. J Orthop Allied Sci 2015;3:4-7.
Abstract
Injuries to pediatric athletes are becoming increasingly common as children compete in more physically demanding sports. These athletic injuries may be acute or as the result of chronic overuse. Acute trauma may lead to damage to tendons, ligaments, and muscles, as well as their bony attachment sites. Infections such as osteomyelitis must also be considered in the differential of pediatric patients presenting with hip or groin pain. This review will discuss the normal muscular attachments to hip physes and physeal equivalents, as well as common injuries and their management. These findings are important to help with the diagnosis and treatment of pediatric patients who present with hip pain.
Keywords
Apophyses
avulsions
physes

Introduction
Development of the pediatric pelvis and hip is complex, with multiple apophyses and physeal equivalents. These apophyses are vulnerable to avulsion in the acute and chronic traumatic settings while their associated physeal equivalents are susceptible to infection due to the increased vascularity during pelvic development. Knowledge of the muscular attachments of the pelvis, predispositions for avulsion injuries with certain sports activities, and suspicion for osteomyelitis in the setting of fever are tantamount for the appropriate diagnosis and treatment of pelvic injury or infection.
Normal Anatomy
Normal developing bones consist of several distinct regions surrounding the growth plate or physis, which contributes to bone lengthening and thickening. The physis itself is not homogenous and has several distinct zones based on their primary function and histological structure. The germinal zone of the physis lies in direct contact with the epiphysis and is composed of loose matrix. It is also called the reserve zone due to the presence of a high density of disorganized chondrocytes which serve as the stem cells of the physis. The proliferative zone lies in the center of the physis and contains organized layers of rapidly-dividing chondrocytes which contribute to lengthening of the bone. The hypertrophic zone is the portion of the physis which abuts the metaphysis and contains enlarged chondrocytes which undergo vacuolization and apoptosis. Within the hypertrophic zone lies another distinct region called the zone of provisional calcification, which delineates the separation between the cartilage of the physis and the bone of the metaphysis.[1] Since the zone of provisional calcification is weaker than previously mineralized bone, it is that part of the growing skeleton which is most susceptible to fractures and injury.[2]
In infants and young children, the epiphysis is a zone of cartilage which lies adjacent to the primary center of ossification.[3] The epiphysis consists of hyaline cartilage organized in several tightly packed layers. These layers undergo ossification and contribute to longitudinal growth of long bones. Together, the epiphysis and physis form the epiphyseal unit. Another critical structure involved in bone elongation is the metaphysis, which lies directly adjacent to the epiphysis. The endochondral ossification which causes growth occurs at this connection zone due to an interaction between the growth plate cartilage and vascular supply of the metaphysis.[4]
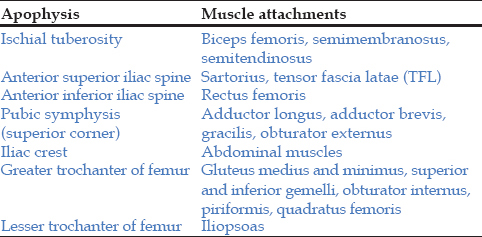
In addition to the normal physis and associated zones, bones may have physeal equivalents or apophyses. These apophyses add to the overall contour of the bone, but do not add significantly to longitudinal growth and serve as muscular attachment sites in the developing child. The pelvis contains several apophyses, including the ischial tuberosity, anterior superior iliac spine (ASIS), anterior inferior iliac spine (AIIS), superior corner of the pubic symphysis, and iliac crest. The lesser and greater trochanter of the femur are also apophyses of the hip, as they serve as muscular attachment sites [Table 1]. These attachment sites are illustrated in Figure 1 Table 1.

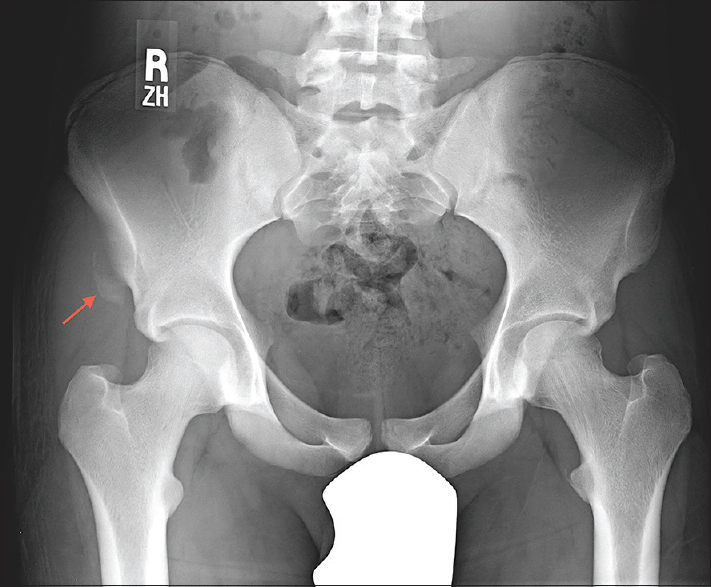
- Illustration and companion radiograph show the bones of the pelvis and hip with physeal equivalents (red) and apophyses (blue). Companion radiograph demonstrates an acute avulsion of the left anterior inferior iliac spine (arrow)
Acute Trauma
Acute trauma may lead to stress on muscles, tendons, and ligaments; ultimately leading to avulsion fractures. Trauma or stress injuries involving different muscles can lead to avulsions of various attachment sites on the pelvis. The abdominal muscles attach to the iliac crest, while the sartorius and tensor fascia lata attach to the ASIS. The rectus femoris attaches to the AIIS, and the gluteus medius and minimus attach to the greater trochanter. Additionally the hip rotators such as the superior and inferior gemelli, obturator internus, piriformis, and quadratus femoris also attach onto portions of the greater trochanter. The lesser trochanter is the attachment site of the iliopsoas. The hamstring muscles (biceps femoris, semimembranosus, and semitendinosus) attach to the ischial tuberosity. The adductor muscles (magnus, longus, and brevis) attach to the body of the pubis and the inferior pubic ramus.[5]
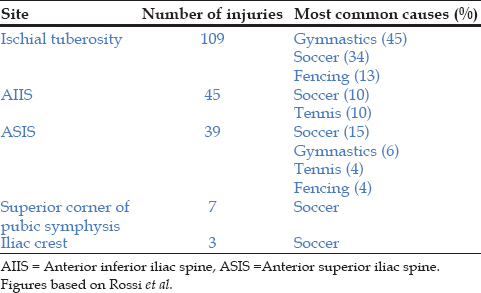
Acute avulsions may present as groin or hip pain depending on the location of the avulsion. The prevalence and locations of the different types of avulsions vary based on several characteristics, including which sports are played by patients. A study by Rossi and Dragoni looked at over 200 cases of avulsion fractures. Of the 203 cases analyzed, over half of the acute injuries resulted in fractures of the ischial tuberosity. Forty-five resulted in AIIS injury, compared to 39 ASIS fractures. The least common fractures were the superior corner of the pubic symphysis and iliac crest. The distribution of injuries also varied by sport type, with gymnastics accounting for the most common cause of ischial tuberosity injuries (45 of 109), followed by soccer (34), and fencing (13). Injuries of the AIIS were most commonly the result of soccer (10 of 45) and tennis (10). ASIS injuries [Figure 2] were most common in patients who played soccer (15 of 39), gymnastics (6), tennis (4), and fencing (4). Soccer accounted for most of the injuries of the superior corner of the pubic symphysis.[6] The findings from Rossi and Dragoni are summarized below in Table 2.
- Pelvic radiograph of a patient with right hip pain shows avulsion of the anterior superior iliac spine which is inferiorly displaced (arrow)
Avulsions of the ischial tuberosity may be caused by hip extension or knee flexion, which places stress on the hamstrings. Avulsions of the iliac crest are commonly caused by a trunk twisting injury, which result in the external and abdominal obliques being stretched. Hip abduction can lead to avulsion of the greater trochanter, whereas, hip adduction can cause damage to the pubic symphysis. Hip flexion by the iliopsoas can lead to avulsions of the lesser trochanter. The first line of treatment for most pelvic avulsion fractions is nonoperative management. One study demonstrated that a five-phase protocol can be applied to treat these fractures. This protocol includes rest and analgesic use for the 1st week after injury, followed by gentle active and passive range of motion. The patient can then begin resistance exercises after 75% of motion is regained. After 1-2 months, sports-specific exercises are started and after at least 2 months after the initial injury, the patient can return to competitive sports.[7]
Surgical management may be undertaken when nonoperative management has been unsuccessful or in acute cases of severe avulsion and distraction. If patients can no longer partake in competitive sports or have persistent symptoms, surgical intervention may be necessary; this is most commonly seen in ischial tuberosity avulsions.[8] If there is fracture with displacement of 2-3 cm, surgery may also be indicated; other indications include painful nonunion and the formation of exostosis.[9] McKinney et al., found that avulsions of the lesser trochanter, iliac crest, and pubic symphysis are rarely treated surgically. Ischial tuberosity injuries, as well as those affecting the greater trochanter, may be treated by open reduction internal fixation (ORIF).[10] ASIS injuries can be treated by a direct incision over the affected area, and AIIS injuries can be treated using a modification of the Smith-Peterson approach.[11]
Chronic Trauma
Chronic trauma, such as repeated insults or a long-standing untreated injury, may cause inflammation. This may be detected as T2 hyperintensity within the apophysis and the physeal equivalent on MRI and termed apophysitis. Frequent microtrauma can lead to avulsions which result in bone formation. In some cases, there may be multiple avulsions in asynchronous stages of healing due to repeated insults of one location. These are generally characteristic of organized sports activities such as cheerleading, sprinting, gymnastics, football, and track.[12] In cases where chronic injury has led to new bone formation, productive bony changes may have an aggressive appearance resembling a neoplastic process or infection.
Infection
Osteomyelitis results if infection spreads to bone, via either hematogenous spread or direct contamination. Pelvic osteomyelitis is rare and may be challenging to clinically diagnose.[13,14] In the pediatric population, pelvic osteomyelitis begins at the physeal equivalent and involves the adjacent pelvic bone and/or apophyses. These areas are thought to be predisposed due to being highly vascularized and are sites for idiopathic hematogeneous or post traumatic seeding. In adults, a history of pelvic or gynecologic procedures is common. Hematogenous spread in pelvic bone infection has also been reported to be associated with urinary tract infections, Crohn's disease, or trauma.[15] It is thought that the ileum is the most common site of bacterial dissemination in the pelvis because it is highly vascularized. Often, there is soft tissue inflammation and abscess adjacent to the focal area of osteomyelitis [Figure 3]. Pain from pelvic osteomyelitis may localize to three main regions. Irritation of the lumbar plexus may result in pain in the hip or back. Formation of a gluteal abscess may result in ilium inflammation and buttock pain. If inflammation of the ilium is extensive, the peritoneum may be affected and present similarly to an acute abdomen. Based on several studies, there seems to be a male predilection. A study by Davidson et al., found that 62% of reported cases affected males. The same study also found that certain areas of the pelvis are more likely to be affected. The areas affected, in decreasing order of prevalence, are the ilium, pubis, ischium, sacrum, ischiopubic ramus, and coccyx. It was also shown that the most common bacterial agent was Staphylococcus aureus, but that negative blood and tissue cultures are also common.[16]
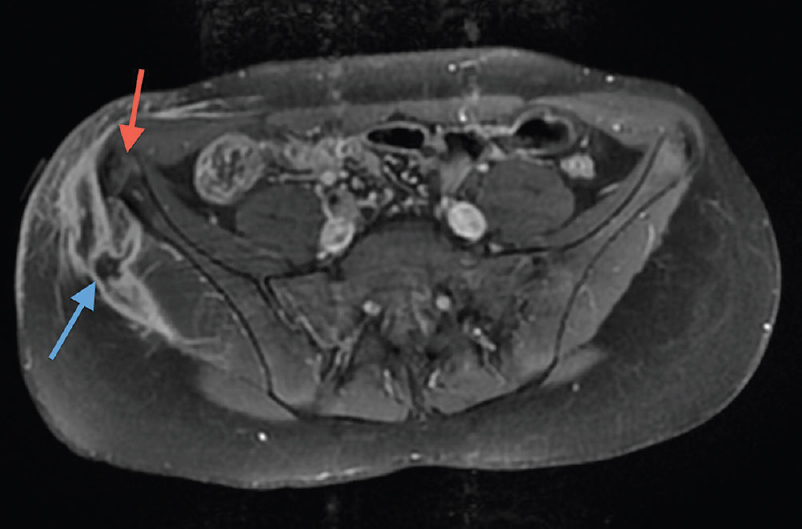
- Axial T1 weighted MRI after gadolinium contrast demonstrates abnormal signal intensity in the right iliac crest apophysis, physeal equivalent and adjacent iliac marrow (red arrow). Rim enhancing fluid collection along the lateral aspect of the right gluteals represents a large abscess (blue arrow)
It may be difficult to differentiate pelvic osteomyelitis from other pediatric syndromes based on clinical features. Pelvic/ hip osteomyelitis should be considered in patients with hip pain or limp with fever, elevated white count, sedimentation rate and C-reactive protein. Abnormal hyperintense T2 signal on MRI within a pelvic physeal equivalent and adjacent bone marrow may indicate chronic trauma (apophysitis) or acute infection.[17] Typically clinical and laboratory information will delineate between the two. In cases with a short clinical history, plain radiographs may not be particularly useful in diagnosis.[12] MRI evaluation, particularly after gadolinium contrast administration is helpful in identifying abscess formation, as well as determining the extent of infection. If MRI indicates severe abscess formation, surgical intervention may be required.[18]
In conclusion, pediatric hip and pelvic pain is a challenging clinical presentation, in part due to the complexity of the developing pediatric hip and pelvis. If musculoskeletal injury or infection is being considered, radiology may be critical to the diagnosis of apophyseal avulsion or physeal equivalent inflammation and infection. Knowledge of the predisposing sports injuries, mechanics, anatomic locations, and imaging appearance on radiographs and cross sectional imaging (particularly MRI) are tantamount to accurate and timely diagnosis.
Source of Support:
Nil
Conflict of Interest:
None declared.
REFERENCES
- Magnetic resonance imaging of pediatric musculoskeletal trauma. Top Magn Reson Imaging. 2002;13:203-17.
- [CrossRef] [PubMed] [Google Scholar]
- Cartilaginous epiphysis and growth plate: Normal and abnormal MR imaging findings. AJR Am J Roentgenol. 1992;158:1105-10.
- [CrossRef] [PubMed] [Google Scholar]
- Metaphyseal abnormalities in children: Pathophysiology and radiologic appearance. AJR Am J Roentgenol. 1993;161:1029-36.
- [CrossRef] [PubMed] [Google Scholar]
- Imaging features of avulsion injuries. Radiographics. 1999;19:655-72.
- [CrossRef] [PubMed] [Google Scholar]
- Acute avulsion fractures of the pelvis in adolescent competitive athletes: Prevalence, location and sports distribution of 203 cases collected. Skeletal Radiol. 2001;30:127-31.
- [CrossRef] [PubMed] [Google Scholar]
- Avulsion fractures of the pelvis. Am J Sports Med. 1985;13:349-58.
- [CrossRef] [PubMed] [Google Scholar]
- Avulsion fractures of the pelvis in children: A report of 32 fractures and their outcome. Skeletal Radiol. 1994;23:85-90.
- [CrossRef] [PubMed] [Google Scholar]
- Avulsion of the ischial apophysis. The case for open reduction and internal fixation. J Bone Joint Surg Br. 1990;72:625-7.
- [CrossRef] [PubMed] [Google Scholar]
- Apophyseal avulsion fractures of the hip and pelvis. Orthopedics. 2009;32:42..
- [CrossRef] [PubMed] [Google Scholar]
- Avulsion fractures of the anterior inferior iliac spine: The case for surgical intervention. Int Orthop. 2001;24:364-5.
- [CrossRef] [PubMed] [Google Scholar]
- MR imaging of septic sacroiliitis. Skeletal Radiol. 2000;29:439-46.
- [CrossRef] [PubMed] [Google Scholar]
- Acute hematogenous osteomyelitis of the pelvis in childhood: Diagnostic clues and pitfalls. Pediatr Emerg Care. 2003;19:29-31.
- [CrossRef] [PubMed] [Google Scholar]
- Pelvic osteomyelitis: A diagnostic challenge in children. J Pediatr Surg. 2007;42:553-7.
- [CrossRef] [PubMed] [Google Scholar]
- Pelvic-femoral osteomyelitis complicating Crohn's disease. Am J Gastroenterol. 1984;79:379-81.
- [Google Scholar]
- Pelvic osteomyelitis in children: A comparison of decades from 1980-1989 with 1990-2001. J Pediatr Orthop. 2003;23:514-21.
- [CrossRef] [PubMed] [Google Scholar]
- MRI for detection of abscess in acute osteomyelitis of the pelvis in children. AJR Am J Roentgenol. 2007;189:867-72.
- [CrossRef] [PubMed] [Google Scholar]
- Pelvic osteomyelitis in children. J Pediatr Orthop B. 2010;19:38-41.
- [CrossRef] [PubMed] [Google Scholar]




