
Translate this page into:
Multisite quantitative ultrasound: It′s comparison with dual energy X-ray absorptiometry in the diagnosis of osteoporosis
Address for correspondence: Dr. Shweta Shenoy, Department of Sports Medicine and Physiotherapy, Guru Nanak Dev University, Amritsar - 143 005. Punjab, India. E-mail: drshweta.sportsmed@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Shenoy S, Chawla JK, Sandhu JS. Multisite quantitative ultrasound: It's comparison with dual energy X-ray absorptiometry in the diagnosis of osteoporosis. J Orthop Allied Sci 2014;2:40-4.
Abstract
Background:
The aim of the study was to establish the correlation between dual-energy X-ray absorptiometry (DXA) and quantitative ultrasound (QUS) and to assess the ability of QUS as a screening tool for osteoporosis.
Materials and Methods:
The study was conducted on 101 healthy women, aged 20-65 years. All the women underwent QUS of radius and tibia using Omnisense bone densitometer and DXA screening for measurement of bone mineral density (BMD) at lumbar spine, total hip, and femoral neck.
Results:
Significant correlations were observed between speed of sound (SOS) and BMD measurement in all age groups, with the closest association. In the age group of 20-40 years, BMD of femoral neck showed the closed association with SOS radius (0.858, P < 0.01) and SOS tibia (0.860, P < 0.01). Similar trend was observed in the other two age groups as well. All subjects in the premenopausal (41-50 years) and postmenopausal (51-65 years) age group were correctly detected for osteopenia/bone density below the expected range for age and osteoporosis by QUS, as against the diagnosis made by DXA. Post hoc test revealed a significant difference in the BMD of femoral neck, lumbar spine, and SOS radius and tibia in young and postmenopausal females.
Conclusion:
QUS is a sensitive screening tool to detect changes in the bone mass and risk of osteoporosis.
Keywords
Dual energy X-ray absorptiometry
osteoporosis
quantitative ultrasound

Introduction
Osteoporosis is a systemic skeletal disease, characterized by low bone mass and microarchitectural deterioration of bone tissue, predisposing to an increased risk of fracture, is a major health problem worldwide.[1,2,3] Worldwide, approximately 200 million women have osteoporosis.[3] In India, for women aged 30-60 years from low-income groups, BMD at all the skeletal sites were much lower than values reported from the developed countries, with a high prevalence of osteopenia (52%) and osteoporosis (29%), thought to be due to inadequate nutrition.[4] Due to rise in rate of osteoporosis, non-invasive methods for skeletal evaluation have been developed, and at present, dual-energy X-ray absorptiometry (DXA) is the most widely used and preferred quantitative technique in the assessment of skeletal status.[1,5] Bone mineral density (BMD) measured by DXA is the best predictor of fracture risk and is currently considered the "gold standard" for diagnosis of osteoporosis,[6,7,8] but it has certain limitations in its clinical or widespread use in comparison with ultrasound.[9] Quantitative ultrasound (QUS) measurement of bone is now increasingly becoming a recognized method of determining bone quality, with review papers written discussing the technique's abilities and usefulness.[10,11,12,13,14] Quantitative ultrasound scanners, in particular, have advantages in that they are portable, less expensive than X-ray-based technologies, do not use ionizing radiation, and do not require a skilled radiographer to perform the measurements.[9] The Sunlight Omnisence™ (Sunlight Medical, Rehovot, Israel) is one such portable QUS machine. It has the capability to scan the distal radius, the proximal phalanx, and the midshaft tibia and supplies results as speed of sound (SOS) (m/s) transmitted through the cortical bone at the measurement site.[9] Both DXA scanners and QUS scanners show results in T-score and Z-score values.
The World Health Organization (WHO) criterion for diagnosis of osteoporosis by BMD measurement is a T-score of <−2.5 or less at the spine, hip, or forearm.[15] A T-score is the number of standard deviations (SDs) by which a patient's BMD deviates from peak bone mass of a young normal population (aged 25-35) of the same race and gender. However, the WHO diagnostic criteria for osteoporosis and osteopenia were derived from studies of postmenopausal Caucasian women[15,16] and should not be used to categorize BMD measurements in young women because they are at much lower risk of fracture. Instead, the International Society for Clinical Densitometry (ISCD) recommends using the Z score, or the number of SDs by which a patient's BMD deviates from a population of the same age, race, and gender to characterize bone mass measurements in premenopausal women.[8] In addition, the ISCD recommends avoiding such terms as osteoporosis and osteopenia when reporting BMD measurements in young women and suggests that young women with BMD Z scores <−2.0 should be categorized as having low BMD or BMD that is below expected range for age, and those with Z scores >−2.0 should be categorized as having BMD that is within the expected range for age.[17] These methods allow for direct comparison of bone status at different measurement sites by using the same analytical approach.[9] Although work has been performed comparing Omnisense for its abilities,[9,18,19] its accuracy in diagnosing osteoporosis still unclear.[20]
Therefore, the aim of this study was to assess the ability of Omnisense device as a screening tool for osteoporosis, and to compare the QUS measurements in radius and tibia with BMD in femoral neck, total hip, and lumbar spine in Asian Indian females.
Materials and Methods
The study sample comprised 101 healthy women. We included a convenience sample of women aged between 20 and 65 years. The protocol was approved by Institutional Ethical Committee of Faculty of Sports Medicine and Physiotherapy, Guru Nanak Dev University, Amritsar. All subjects signed the informed consent form. The exclusion criteria for healthy pre- and postmenopausal women included a menopause before the age of 45; amenorrhea for 6 or more months, a history of drugs or diseases known to affect bone metabolism; or a history of low trauma fracture.[21] The subjects were recruited from Guru Nanak Dev University campus. The study was conducted in Faculty of Sports Medicine and Physiotherapy, Guru Nanak Dev University, Amritsar. The study population was divided into three groups: (1) Young normals (20-40 yrs), (2) healthy premenopausal (41-50 yrs), (3) and healthy postmenopausal (51-65 yrs).[18,19] All subjects underwent DXA screening followed by SOS measurement with Omnisense using standard protocol as follows.
Subject measurement
The Omnisense uses a hand-held probe to make SOS measurements at the phalanx, radius, tibia, or metatarsal. The probe contains a number of transducers, some acting as transmitters and the others as receivers. The device uses Fermat's principle[22] to identify the path of the sound wave taking the shortest time to pass between the transmitting and receiving transducers. The exact path of the signal is determined by Snell's law:[22] As it enters the bone from the soft tissue the signal is refracted through a critical angle that is a function of the ratio of the SOS in soft tissue and bone. After it propagates along the bone, the sound wave emerges at the same critical angle. The time taken for the signal to travel between the transmitting and receiving transducers is used to infer the SOS in bone.[23] Speed of sound measurements were performed at the non-dominant medial aspect of the one-third radius, anteromedial aspect of the midshaft tibia using the Omnisense.[19] One probe was used to measure both radius and tibia.[24] DXA Hologic Discovery Wi was used for bone density at femoral neck and lumbar spine. The scans were analyzed with the most recent software APEX version 4.0. The scan measurements and analyses were conducted following standard analysis protocol as described in the Hologic User Manual. All scans were subsequently analyzed by a single trained investigator.[25] The Sunlight Omnisense™ and the Hologic Discovery Wi adhere to the levels set out by the WHO.[26]
Statistical analysis
Pearson's correlation coefficient was used to evaluate the association between SOS and BMD measurement using SPSS version 17.0.
Using the selected variables including the values of BMD neck of femur, SOS radius, and SOS tibia from our study, the average effect size (f) computed was 0.72, and with α error of probability to be 0.05, the power of the current study was found to be above 90%, using G software version 3.1.2.
Healthy postmenopausal women were classified into three groups according to their T-scores, based on the WHO criteria: Normal, T≥−1.0; osteopenic-1.0 >T>−2.5; osteoporotic T ≤−2.5.[18] For young normal and premenopausal women, Z-score for neck of femur (N.O.F), radius, and tibia was considered for bone health assessment based on ISCD guidelines for identification women with bone density below the expected range for age (Z-score<−2.0).[17]
Results
The subject characteristics according to age groups are shown in Table 1. Correlation between DXA and QUS sites is shown in Table 2.

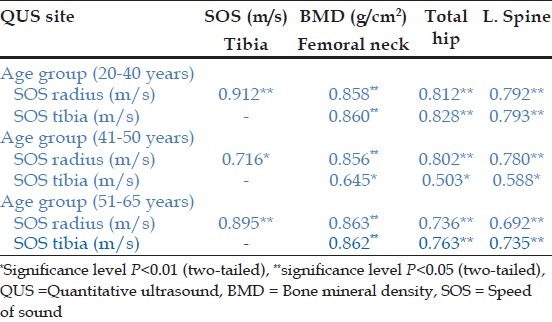
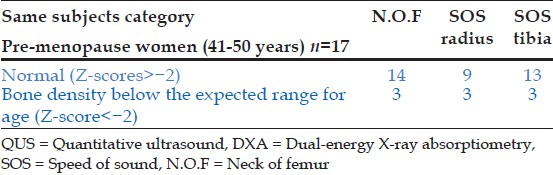
Significant correlations were observed between SOS and BMD measurements. Speed of sound of radius and tibia was correlated with BMD measurement of three sites [N.O.F, total hip (TOT. HIP), and L1-L4 spine; Table 2]. In young females (20-40 years), SOS of radius and tibia were significantly correlated with all the three sites. In the young normal age group (20-40 years), among the three sites, BMD N.O.F showed the closest association with SOS radius (r = 0.858) and SOS tibia (r = 0.860) measurements Table 2. Similar trend of association was observed in the other age groups i.e. (41-50 and 51-65 years) as well. Significant correlations were also noted in between SOS sites measurement in all the age groups Table 2. In screening for osteoporotic females in the postmenopausal group (T-score < −2.5), T-scores obtained by SOS values from both the sites (radius and tibia) were able to identify all the patients correctly (100%) as against the diagnosis made by gold standard DXA [Table 3]. In the same group, for the identification of osteopenic females (T-score < −1and >−2.5), QUS measurement of radius correctly identified 71.9% of the total subjects, whereas measurements at tibia identified 59.38% of population as against the T-scores of N.O.F obtained by DXA [Table 3]. Further, in the premenopausal group, QUS measurements done at the radius and tibia correctly identified all the subjects (100%) with bone density below the expected range for age when compared with DXA [Table 4]. Similarly, comparison of Z-scores of radius and tibia was done with Z-scores of N.O.F to evaluate the capability of QUS in identification of bone density below the expected range for age (Z-score <−2) in healthy young normal and premenopausal women. It was found that QUS measurement of radius identified all the subjects (100%) correctly, whereas measurements done at the tibia identified 81.8% of the population as against the diagnosis made by DXA [Table 5]. Also, post hoc Scheffe's test was done to observe multiple comparisons between groups. Significant differences were noted in the BMD N.O.F, BMD lumbar spine, and in both the SOS sites radius and tibia between young and postmenopausal groups [Table 6]. However, non-significant differences were observed between premenopausal and postmenopausal groups and premenopausal and young normal groups.



Discussion
The primary objective of the study was to evaluate the ability of QUS (Omnisense) in the screening of osteopenia, osteoporosis, and bone density below the expected range for age in postmenopausal, premenopausal, and young normal females, respectively, in comparison to DXA in Asian Indian population.
The QUS and DXA devices are based on two distinctly different technologies and measure two different parameters; SOS and BMD. QUS performs measurements of predominantly cortical bone. However, because the diagnosis of osteoporosis concerns assessment of fracture risk and not assessment of bone mass, there is, indeed, a basis for comparison.[27]
Results from this study demonstrate significant correlation between SOS and BMD sites. The strongest correlation was found between SOS radius and BMD N.O.F in all the three age groups Table 2. Literature suggests that traditional DXA is limited to measuring one property only, i.e. BMD.[27] It measures the areal BMD of the cortical bone and the medullary cavity conversely, whereas the QUS using SOS measurements gives a much broader perspective reflecting several varied bone properties, such as density, elasticity, cortical thickness, and micro-architecture, thus providing a more complete picture of the bone's fragility.[28,29] Apart from detecting bone changes and determining fracture discrimination, QUS advantage also includes its applicability of WHO criteria for postmenopausal women.[30]
The mean difference in the values of SOS (m/s) and BMD (gm/cm2) at all measured sites [Table 1] was significantly different between postmenopausal and pre menopausal women indicating that the loss of the bone in these detected women is indeed significant. The fact that QUS detected these differences as statistically significant, indicating that it is sensitive to detect these changes [Table 6]. Our results are supported by the findings of Knapp et al. (2001), who also observed a similar trend in his study. Considering the diagnosis of osteoporosis in the postmenopausal group, we also observed the ability to identify osteoporosis with use of WHO criteria in comparison to DXA. It was found that QUS SOS measurements were sensitive enough to correctly identify all four cases of osteoporosis diagnosed using N.O.F BMD values on DXA. These patients were correctly identified by using T-scores, obtained by SOS measurements at radius as well as at tibia [Table 3]. Further, 32 subjects were diagnosed as osteopenic of N.O.F by DXA, though T-scores of SOS tibia correctly identifies 19 of these subjects and T-scores of SOS radius identified 23 subjects correctly [Table 3]. Thus, as a screening tool for osteoporosis, it is accurate. However, T-score of SOS radius can identify majority of women (71.8%) of women with osteopenia but not all cases of osteopenia. The greater number of subjects identified by SOS radius indicates a clear demarcation between the bone loss at the weight-bearing and non-weight-bearing ultrasound sites may be due to the positive effects of weight-bearing activity on reducing bone loss.[6] A previous research by Knapp et al. (2001) suggested that the QUS SOS measurements of the radius are equal to or superior than DXA in predicting wrist fracture patients from controls (odds ratio of 2.4; 95% C.I. 1.2-5.0, compared to odds ratio <2.0 of DXA of L1-4, N.O.F, and total hip.
This picture is made clear from Tables 4 and 5 where Z-scores obtained from SOS radius identified all the subjects with bone density below the expected range for age in the young normal and premenopausal women as against the gold standard DXA.
Clearly Z-scores and T-scores obtained from SOS radius are sensitive to changes in the bone mass and should be used as an early screening tool for detecting changes in bone mass. But these scores cannot be extrapolated to other sites like phalanges and calcaneum.
Therefore, the results of our study confirm QUS to be an accurate screening tool in identifying patients at risk of osteoporosis. It has the capability to differentiate between young, pre- and postmenopausal females and can serve as an alternative to the traditional radiation-based technologies.
Source of Support:
Results are a part of major research project entitled “Nutrition and Bone health in Punjab: A community study” Funded by Department of Science and technology, Ministry of Science and technology, New Delhi-110026. DST Ref no: SSD/WD/012/2010/GNDU.
Conflict of Interest:
None declared.
REFERENCES
- How can we measure bone quality? Baillière's Clin Rheumatol. 1997;11:495-515.
- [CrossRef] [PubMed] [Google Scholar]
- Guidelines for diagnosis and management of osteoporosis. The European Foundation for Osteoporosis and Bone Disease. Osteoporos Int. 1997;7:390-406.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology, etiology, and diagnosis of osteoporosis. Am J Obstet Gynecol. 2006;194:S3-11.
- [CrossRef] [PubMed] [Google Scholar]
- Bone status of Indian women from a low-income group and its relationship to the nutritional status. Osteoporos Int. 2005;16:1827..
- [CrossRef] [PubMed] [Google Scholar]
- The ultrasonic assessment of osteopenia as defined by dual X-ray absorptiometry. Br J Radiol. 1994;67:631-5.
- [CrossRef] [PubMed] [Google Scholar]
- Ultrasound velocity and attenuation at different skeletal sites compared with bone mineral density measured using dual energy X-ray absorptiometry. Br J Radiol. 1996;69:25-32.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation of femoral and lumbar DXA and calcaneal ultrasound, measured in situ with intact soft tissues, with the in vitro failure loads of the proximal femur. Osteoporos Int. 1998;8:591-8.
- [CrossRef] [PubMed] [Google Scholar]
- Quantitative heel ultrasound as a predictor for osteoporosis. Med J Aust. 1999;171:297-300.
- [CrossRef] [PubMed] [Google Scholar]
- The ability of peripheral quantitative ultrasound to identify patients with low bone mineral density in the hip or spine. Ultrasound Med Biol. 2005;31:625-32.
- [CrossRef] [PubMed] [Google Scholar]
- Perspectives: Ultrasound assessment of bone. J Bone Miner Res. 1993;8:517-25.
- [CrossRef] [PubMed] [Google Scholar]
- Quantitative ultrasound techniques for the assessment of osteoporosis: Expert agreement on current status. J Bone Miner Res. 1997;12:1280-8.
- [CrossRef] [PubMed] [Google Scholar]
- The epidemiology of quantitative ultrasound: A review of the relationships with bone mass, osteoporosis and fracture risk. Osteoporos Int. 1997;7:89-99.
- [CrossRef] [PubMed] [Google Scholar]
- The diagnosis of osteoporosis. J Bone Miner Res. 1994;9:1137-41.
- [CrossRef] [PubMed] [Google Scholar]
- Diagnosis of osteoporosis and assessment of fracture risk. Lancet. 2002;359:1929-36.
- [CrossRef] [PubMed] [Google Scholar]
- Special report on the official positions of the International Society for Clinical Densitometry. Osteoporos Int. 2004;15:779-84.
- [CrossRef] [PubMed] [Google Scholar]
- Premenopausal bone health assessment. Curr Rheumatol Rep. 2005;7:46-52.
- [CrossRef] [PubMed] [Google Scholar]
- Can the WHO definition of osteoporosis be applied to multi-site axial transmission quantitative ultrasound? Osteoporos Int. 2004;15:367-74.
- [CrossRef] [PubMed] [Google Scholar]
- Multisite quantitative ultrasound: Precision, age-and menopause-related changes, fracture discrimination, and T-score equivalence with dual-energy X-ray absorptiometry. Osteoporos Int. 2001;12:456-64.
- [CrossRef] [PubMed] [Google Scholar]
- The role of quantitative ultrasound in predicting osteoporosis defined by dual X-ray absorptiometry. Rheumatol Int. 2001;20:55-9.
- [CrossRef] [PubMed] [Google Scholar]
- Postmenopausal screening of osteopenia. Br J Rheumatol. 1992;31:823-8.
- [CrossRef] [PubMed] [Google Scholar]
- A new method for quantitative ultrasound measurements at multiple skeletal sites. J Clin Densitom. 2000;3:1-7.
- [CrossRef] [PubMed] [Google Scholar]
- An assessment of the use of quantitative ultrasound and the Osteoporosis Self-Assessment Tool for Asians in determining the risk of nonvertebral fracture in postmenopausal Chinese women. J Bone Miner Metab. 2008;26:60-5.
- [CrossRef] [PubMed] [Google Scholar]
- Longitudinal body composition changes in old men and women: Interrelationships with worsening disability. J Gerontol A Biol Sci Med Sci. 2007;62:1375-81.
- [CrossRef] [PubMed] [Google Scholar]
- The role of ultrasound assessment of osteoporosis: A review. Osteoporos Int. 1997;7:7-22.
- [CrossRef] [PubMed] [Google Scholar]
- 1998 Sunlight Omnisense™ User Manual. Tel Aviv, Israel: Sunlight Ultrasound Technologies;
- [Google Scholar]
- QUS Derived Speed of Sound and Cortical Bone Structure. (abstract) presented at the ASBMR 21st Annual Meeting in St. Louis, MI, USA, September 1999
- [Google Scholar]
- An in vitro Investigation of the dependence on sample thickness of the speed of sound along the specimen. Med Eng Phys. 1999;21:651-9.
- [CrossRef] [PubMed] [Google Scholar]
- Reference database for bone speed of sound measurement by a novel quantitative multi-site ultrasound Device. Osteoporos Int. 2000;11:688-96.
- [CrossRef] [PubMed] [Google Scholar]




