
Intraosseous diffuse large B-cell lymphoma presenting as fracture of humerus
Address for correspondence: Dr. Prakas Kumar Mandal, 8c/1/N, Roy Para Road, First Floor, Kolkata 700 050, West Bengal, India. E-mail: prakas70@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Dolai TK, Mandal PK. Intraosseous diffuse large B-cell lymphoma presenting as fracture of humerus. J Orthop Allied Sci 2014;2:24-5.
Abstract
Non-Hodgkin's lymphomas (NHL) is the most common primary bone lymphoid malignancy, and diffuse large B-cell lymphoma (DLBCL) accounts for the greatest percentage of cases. Here we report a 34-year-old male presented with pain and swelling of left shoulder joint of 2-month duration. There was no history of trauma. A diagnosis of intraosseous NHL-Diffuse large B-cell lymphoma (DLBCL) was made. He was treated with six cycles of with R-CHOP (Rituximab, Cyclophosphamide, Vincristine, Doxorubicin and Prednisolone) chemotherapy. Our report suggests that primary intraosseous high-grade NHL, e.g. DLBCL can present as fracture in an unusual site in a young adult.
Keywords
Chemotherapy
diffuse large B-cell lymphoma
fracture of humerus

Introduction
Primary intraosseous lymphoma is a rare type of lymphoma accounting for about 5% extranodal lymphoma.[1] The authors report a patient with primary intraosseous diffuse large B-cell lymphoma (DLBCL) presenting as fracture of humerus.
Case Report
A 34-year-old male presented with pain and swelling of left shoulder joint of 2 -month duration. The patient complained of severe pain in the night and unable to raise the left upper extremity in the morning. There was no history of fever, weight loss, fatigability, weakness and swelling of any lymph gland. No past and present history of injury or trauma to left arm.
Examination revealed diffuse swelling, tenderness of left shoulder joint and weakness of left upper extremity without anemia, lymphadenopathy, or any organomegaly.
Hemogram was normal. Liver function test and serum chemistries were normal except slightly elevated LDH 442 U/l and serum β2 microglobulin (2164.1 mcg/l). HBsAg, anti-HCV antibody, and anti-HIV-I and II were non-reactive. Straight X-ray of left shoulder joint [Figure 1] revealed fracture of upper part of left humerus with significant osteolytic lesions; MRI showed fracture and intraosseous thickening.

- Straight X-ray of left shoulder joint revealed fracture of upper part of left humerus with significant osteolytic lesions
Biopsy from humerus with histopathology [Figure 2] revealed that bony trabeculae are intervened by fibrotic and desmoplastic marrow spaces with sheets of atypical lymphoid cells; composed of medium to large cells with hyperchromatic nuclei. Brisk mitosis was noted. The features were suggestive of non-Hodgkin's lymphoma (NHL) with diffused large cell type. The tumor cells expressed CD20, CD45, BCL6, and BCL2 and were negative for CD3, Alk-1, CD15, cytokeratins and Ki-67 was 78%. Post-biopsy wound was healthy [Figure 3]. Bone marrow aspiration and biopsy was normal. Contrast-enhanced computer tomography (CECT) of neck, chest, abdomen, and pelvis was normal.
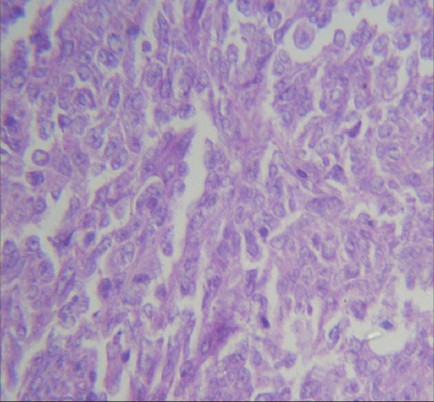
- Biopsy from humerus with histopathology revealed non-Hodgkins' lymphoma-diffuse large cell type (×40 magnification)

- Post-biopsy, wound was healthy
Diagnosis of intraosseous NHL-Diffuse large B- cell lymphoma (DLBCL) was made. After counseling, chemotherapy with Rituximab, Cyclophosphamide, Vincristine, Doxorubicin and Prednisolone (R-CHOP) 21-day interval was started. After the 6th cycle of chemotherapy, positron emission tomography (PET-CT) did not reveal any metabolically active disease. Patient was sent to orthopedic surgeon for reconstructive surgery.
Discussion
Non-Hodgkin lymphoma is the most common primary bone lymphoid malignancy, and diffuse large B-cell lymphoma accounts for the greatest percentage of cases.[2,3] The most common presentation of these patients is bone pain, and some have the initial presentation of a palpable mass.[2] In contrast to the classical manifestations of patients with non-bone lymphoma, symptoms, including fever, loss of body weight and night sweating, are rarely noted among patients with primary bone lymphoma.[4] In the present case, the authors demonstrated an atypical presentation of fracture of humerus without any definite history of trauma in a patient of intraosseous DLBCL. Qureshi et al.[2] reviewed a total of 60 cases of bone lymphoma, the most common site of involvement was femur (28.3%), followed by hip (16.6%) and humerus (10%), thus making humerus an unusual site of presentation especially in a young adult, as in our case. Diffuse large B-cell lymphoma of bone, mostly reported in the age of 60 years and above.[2] Patients with bone lymphoma, shown to have good outcome and responded well to chemotherapy.[5]
Our report suggests that primary intraosseous high grade NHL, e.g. DLBCL can present as fracture in an unusual site in a young adult.
Source of Support:
Nil
Conflict of Interest:
None declared.
REFERENCES
- Primary lymphoma of bone. A B-Cell neoplasm with a high frequency of multilobated cells. Am J Surg Pathol. 1990;14:329-34.
- [CrossRef] [PubMed] [Google Scholar]
- Primary non-hodgkin's lymphoma of bone: Experience of a Decade. Indian J Pathol Microbiol. 2010;53:267-70.
- [CrossRef] [PubMed] [Google Scholar]
- Primary non-Hodgkin's lymphoma of bone: A single institution experience. Med Oncol. 2004;21:263-7.
- [CrossRef] [PubMed] [Google Scholar]
- Intraosseous lymphoma presenting as a fracture of the femoral neck. Int J Case Rep Med 2013:2013.
- [CrossRef] [Google Scholar]
- Primary lymphoma of bone an institutional experience. Leuk Lymphoma. 2008;49:2125-32.
- [CrossRef] [PubMed] [Google Scholar]




