
Translate this page into:
Candida-septic arthritis in an immunocompetent male child: Report of a rare occurrence
Address for correspondence: Dr. Kavita Mardi, 12 A, Type V Quarters, GAD Colony, Kasumpti, Shimla, Himachal Pradesh, India. E-mail: kavitamardi@yahoo.co.in
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Mardi K, Sharma R. Candida-septic arthritis in an immunocompetent male child: Report of a rare occurrence. J Orthop Allied Sci 2014;2:12-3.
Abstract
Systemic candidiasis is usually associated with immunosuppression. Fungal arthritis due to candidal organism in an immunocompetent patient is rare. We describe one such rare occurrence in a young boy without any predisposing factors, who developed knee arthritis caused by Candida albicans.
Keywords
Candida
child
immunocompetent
septic arthritis

Introduction
Septic arthritis is a relatively common disease. But those caused by fungi are rare.[1] Fungal arthritis is usually associated with predisposing conditions that reduce cellular immunity. In children also candidiasis is usually associated with immunosuppression. Candida arthritis in an immunocompetent child is rare.[2,3,4,5] We describe one such rare occurrence in an 11-year-old immunocompetent male child.
Case Report
An 11-year-old male child presented with pain in right knee and distal thigh. He also complained of fever and inability to walk since 5 days. There was no history of injury to the site. On examination, right lower leg was in flexion at knee joint. The right knee joint was swollen and painful. The temperature over distal thigh and knee was raised. X-ray showed evidence of multifocal radiolucent lesion in the distal end of femur involving the metaphyses and epiphyses. These lesions were irregular in outline and surrounded by sclerosis. Similar lesion involves the upper end of tibia.
Magnetic resonance imaging (MRI) showed heterogenously enhancing lesion in distal femur with involvement of metadiaphysis and extending into the epiphysis with joint effusion [Figure 1]. A clinical diagnosis of acute osteomyelitis right distal end of femur with septic arthritis right knee was made. Right knee exploration with lavage, debridement, knee arthrotomy, and intramedullary decompression was done. Postoperatively the patient was put on intravenous ceftrioxone and amikacin. But the patient did not show much improvement. Synovial biopsy was done and sent for histopathological examination. Microscopic examination revealed synovial tissue covered by fibrinopurulent exudates containing fungal colonies comprising pseudohyphae and spores of candidal species, which were periodic acid-Schiff (PAS) positive [Figure 2]. Synovial fluid was aspirated and sent for culture studies that confirmed the presence of Candida albicans in the joint fluid. Treatment with amphotericin B was initiated, which was changed to fluconazole 3-weeks later.

- MRI showed hetereogenously enhancing lesion in distal femur, extending into the epiphysis with joint effusion. MRI = Magnetic resonance imaging
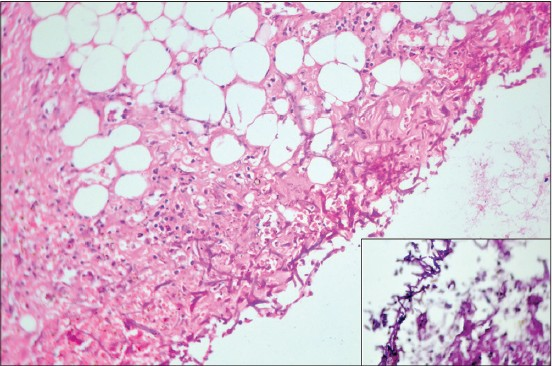
- Synovial tissue covered by fibrinopurulent exudates containing fungal colonies of C. albicans (H and E, ×40), inset shows PAS-positive fungal colonies (PAS stain, ×40). H and E = Hematoxylin and eosin, PAS = Periodic acid-Schiff
Discussion
Fungal arthritis is a rare condition.[2,3,4,5] It can be caused by any of the invasive types of fungi. These organisms may affect bone or joint tissue. One or more joints may be affected by fungal arthritis and most often the large weight-bearing joints, especially the knee joints are affected. Fungal infections that can cause fungal arthritis include blastomycosis, candidiasis, coccidiomycosis, cryptococcosis, histoplasmosis, and sporotrichosis. The infection sometimes occurs as a result of an infection in another organ such as the lungs and tends to involve joints slowly.
Invasive Candida infections tend to occur in patients who are immunocompromised (e.g. neutropenia and glucocorticoid therapy). Patients who develop septic arthritis with Candida usually have predisposing factors such as treatment with broad spectrum antibiotics[6] or steroids,[6] immunosuppressive therapy,[6] malignancy,[6] rheumatoid arthritis,[7] joint aspiration, or arthroplasty.[8]
C. albicans is the most common candidal organism causing fungal arthritis. But other species such as C. glabrata, C. parapsilosis, and C. tropicalis can also cause arthritis.[9] Romero et al.,[10] described a case of Candida-septic arthritis of the knee in an immunocompetent patient who was not a drug abuser and who had no other predisposing factors. The signs and symptoms of Candida-septic arthritis differ from those of other causes of septic arthritis. Pain and swelling are present in all patients but fever, warmth, and erythema are rare in those with Candida-septic arthritis. The knee is more frequently involved than the hip or shoulder.[9]
The clinical diagnosis of septic arthritis due to Candida may be difficult because of the absence of specific signs and symptoms and the unusual nature of the organism. However, the presence of a positive culture for Candida in the synovial fluid should not be interpreted as a contaminant,[7,9] as this delays diagnosis and treatment. β-D-glucan is a constituent of fungi, and elevated plasma levels are common in patients with mycosis or fungemia. Serological kits with proven clinical application have been developed for the rapid diagnosis of mycoses.
The treatment of candida arthritis has not been established. The response to fluconazole is variable. Successful treatment with amphotericin B has been more reported.
Source of Support:
Nil
Conflict of Interest:
None declared.
REFERENCES
- Septic arthritis due to Scedosporium apiospermum: Case report and review. J Infect. 2001;43:210-2.
- [CrossRef] [PubMed] [Google Scholar]
- Fungal septic arthritis in an immunocompetent girl. Pediatr Rheumatol Online J. 2012;10:39..
- [CrossRef] [Google Scholar]
- Remitting septic arthritis due to albicans candida in an immunocompetent subject. Tunis Med. 2011;89:573..
- [Google Scholar]
- Arthritis caused by Candida in an immunocompetent infant with a history of systemic candidiasis in the neonatal period. An Pediatr (Barc). 2003;70:383-5.
- [Google Scholar]
- Candida arthritis after arthroscopic arthroplasty in a patient without predisposing factors. Open Rheumatol J. 2010;11:7-9.
- [CrossRef] [PubMed] [Google Scholar]
- Vertebral osteomyelitis due to candida species: Case report and literature review. Clin Infect Dis. 2001;33:523-30.
- [CrossRef] [PubMed] [Google Scholar]
- Infection with Candida albicans of a total knee arthroplasty: Case report and review of the literature. Clin Orthop. 1988;226:235-9.
- [CrossRef] [Google Scholar]
- Candida arthritis in adult patients who are not intravenous drug addicts: Report of three cases and review of the literature. Semin Arthritis Rheum. 1993;22:224-41.
- [CrossRef] [PubMed] [Google Scholar]
- Candida arthritis in an immunocompetent patient without predisposing factors. Clin Rheumatol. 1998;17:393-4.
- [CrossRef] [PubMed] [Google Scholar]




