
Translate this page into:
Is intraarticular administration of tranexamic acid better than its intravenous administration in reducing blood loss after total knee arthroplasty?
Address for correspondence: Dr. Parag Garg, 145 Rajendra Nagar, Lucknow, Uttar Pradesh, India. E-mail: pgiluvu@gmail.com
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
How to cite this article: Pispati A, Garg P, Patil N, Savedekar A, Jaiswal N, Kumar A. Is intraarticular administration of tranexamic acid better than its intravenous administration in reducing blood loss after total knee arthroplasty?. J Orthop Allied Sci 2013;1:28-32.
Abstract
Context:
It has been well-established now that intravenous (IV) tranexamic acid (TXA) is a potent agent to control postoperative blood loss following total knee arthroplasty (TKA). Recently, intraarticular administration of this agent has also shown good efficacy for the same.
Aims:
Comparison of postoperative blood loss between IV and topical administration of TXA in TKAs.
Materials and Design:
Eighty-six TKAs on knees were included in this study. Randomization was done so that 40 TKA received 1 g of IV TXA, while 46 had intraarticular administration of 1 g TXA.
Subjets and Methods:
We compared the postoperative blood loss by calculating the difference in pre- and postop hemoglobin and need for blood transfusion. Functional assessment was done on basis of Western Ontario McMaster Osteo-Arthritis Index (WOMAC) scores and complications like postoperative infection, oozing from the wound site and thromboembolic manifestations.
Results:
Blood loss was significantly less in the intraarticular administration group as compared to the IV injection group. Total blood loss, blood transfusion group, and drain output was also less but the difference was not significant. The functional assessment (WOMAC) scores were equivocal and so were the complications including thromboembolic manifestations (two cases each of deep vein thrombosis (DVT) and no cases of pulmonary embolism (PE)).
Conclusion:
Intraarticular administration of TXA to prevent postoperative blood loss in TKA is a safe and effective alternative/adjunct to its IV administration.
Keywords
Intraarticular administration
tranexamic acid
total knee arthroplasty

Introduction
Tranexamic acid (TXA) has been a revelation for arthroplasty surgeons in the recent past helping them to giving reduce postoperative blood loss, especially in total knee arthroplasty (TKA). Numerous studies and trials have now proven the efficacy and safety of this drug.[1,2,3,4,5,6,7,8,9,10,11,12,13,14] Additional advantages of this drug are good availability, affordability, and easy administration. Traditionally an intravenous (IV) dose in various doses has been used by various surgeons and their results have been extensively studied.[3,4,5,6,7,8,9,10,11,12,13,14] Oral TXA also has been shown to have equal efficacy by Zohar et al.[1] Recently, there has been a growing interest in intraarticular administration of TXA for TKA. Wong et al.,[2] and many others[6,7,8] have shown good results for intraarticular administration of this drug in TKA. But all of them have compared intraarticular administration of TXA with placebo controls. Hence, it is difficult to conclude whether the drug actually acts locally or gets absorbed systemically and then acts like an IV agent. To clear these doubts and to confirm the efficacy of topical administration of this drug, we have here performed a comparative study between topical and IV administration of TXA in TKAs.
Materials and Methods
This study was conducted during a period of 1 year, from June 2010 to July 2011. Our inclusion criteria were all patients undergoing uncomplicated unilateral TKA for primary osteoarthritis consenting to be a part of this study. Exclusion criteria was allergy to TXA, preoperative anemia (hemoglobin less than 11 g/dL in males and less than 10 g/dL for females), history of use of any form of anticoagulant therapy in the period of 5 days before surgery, coagulopathy (determined by platelet count less than 150,000; international normalized ratio (INR) > 1.4; history of throboembolic disease), and other comorbidities like renal (creatinine > 1.5 g/dL) and cardiovascular compromise (New York Heart Association class III or IV). Complicated deformities requiring a stem, wedge, or revision components were not included in this study.
All patients were duly informed about the study that they were going to be a part of, its risks and advantages and all of them consented to it. A computer generated stratified randomization was used to select patients for the mode of administration and this was not revealed to the operating surgeons team. At the end of 1 year, 86 patients were included in this study, 40 of them received IV administration while 46 topical administration of TXA. An equal dose of 1 g of TXA was used for both modes of administrations.
A similar protocol of surgical management was used for both the groups. All patients were operated under epidural anesthesia, with tourniquet control of 300 Hg pressure. Crystalloids in the form of normal slaine (NS) and dextrose normal saline (DNS) were used as maintenance fluids. All operations were performed by one senior surgeon (AP) along with his operating team. A standard midline incision with medial parapatellar approach was used for all the surgeries. Standard techniques of intraoperative hemostasis were used. All knees were implanted with a posterior stabilized (PS) cemented knee (Either Exactech or Zimmer). Tourniquet was released after cementing and careful hemostasis achieved. Wounds were closed in layers over a 12 gauge suction catheter but it was not opened until 1 h after the surgery.
IV TXA was administered 10 min before the tourniquet was inflated as an infusion in the running drip. On the other hand intraarticular administration was done by injecting 1 g of TXA mixed with 10 mL of NS in the knee joint after closure of the wounds.
Postoperative protocol was also similar for both of the groups. A standard prophylaxis against venous thromboembolism in the form of subcutaneous injections of low molecular weight heparin (LMWH; enoxaparin 40 mg) was given to all patients once daily from day 1 postop till 7 days postop. Postop evaluation consisted of daily hemoglobin level for the first 3 days along with packed cell volume (PCV). The drain was removed routinely 48 h after surgery and drain output measured every 8 hourly. Blood transfusion was deemed necessary only if postop hemoglobin was < 8 mg/dL or even at > 8 g/dL if the patient developed intolerable symptoms of anemia, not attributable to any other causes recommended by American Society of Anesthesiologists (ASA) task force.[15] One unit of blood was transfused at a time, till we expected a recovery of hemoglobin above 8, and the tests confirmed it. Total blood loss was calculated using these values the formula prescribed by Good et al.,[17] and Nadler et al.[20] [Figure 1]. Incidence of surgical infections, oozing from wound site, and time of stitch removal also was carefully noted. Functional evaluation was done using the Western Ontario McMaster Osteo-Arthritis Index (WOMAC) scores. Pre- and postoperative (2nd day) diagnostic Doppler ultrasound examination was done for both legs of the patient to evaluate for any deep vein thrombosis (DVT). All thromoembolic events were duly recorded till 12 weeks follow-up of the patient.

- Calculation of postoperative blood loss on the basis of hemoglobin balance according to equations described by Good, et al., and Nadler, et al.
Statistical analysis used
Statistical Package for Social Sciences (SPSS) 18.0 (Windows, NY) was used for all analysis. A student's t-test was used to compare the demographics and results of the two groups. P of < 0.05 was taken as significant.
Results
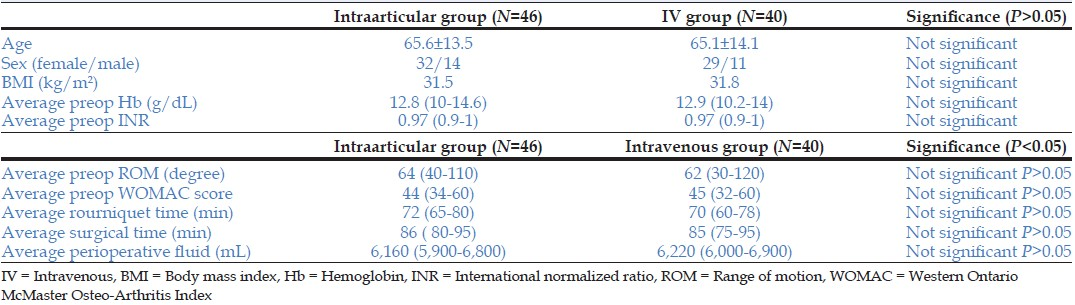
We took 6 months as the minimum follow-up for evaluation of these results and all 86 patients were successfully followed up for this duration. There was no significant difference in sex, age, body mass index (BMI), preoperative hemoglobin, and INR of the two groups [Table 1]. The average tourniquet time and surgery time for both the groups was similar. The amount of perioperative fluid given was also comparable for both groups [Table 1]. The preoperative range of motion (ROM), knee flexion, and WOMAC scores were also comparable for both groups.
The average decrease in hemoglobin was significantly more for the IV group (average 1.6 g/dL, range 0.8-2.8 g/dL) than the topical administration group (0.9 g/dL, range 0.4-2.0 g/dL) (P < 0.05, significant). There was also reduction in blood loss for the topical administration of TXA (average 1,020; range 650-1,550 mL) as compared to the IV group (average 1,205 mL, range 800-1,650 mL) although this was not significant (P > 0.05). Blood transfusion rate was more for the IV group (7/40 (17.5%), total 12 units, 0.3 units/patient, range 0-2) as compared to the topical group (6/46 (13%), total 9 units, 0.2 units/patient, range 0-2), but not significant (P > 0.05). Similarly, the total drain output was more in the IV group (average 350 mL) as compared to the topical group (average 260 mL; P > 0.05) [Table 2].

Postoperatively there was oozing from the wound site in 4/40 patients (10%) in the IV group and 3/46 patients (6.5%) in the topical group. The average time of stitch removal was similar in both groups (14 days, range 12-16 days). There was evidence of postoperative infection in two cases each of the IV (0.5%) and topical group (0.43%) [Table 3].

There was no significant difference in postop ROM and WOMAC scores of the two groups [Table 3]. There was also no difference in incidence of thromboembolictic findings (two cases each of DVT for topical (0.43%) and IV group (0.5%) and no cases of symptomatic pulmonary thromobembolism in either of the groups).
Discussion
In the last decade or so there have been numerous trials, studies, and meta-analysis to evaluate TXA as a new means of chemo-hemostasis.[1,2,3,4,5,6,7,8,9,10,11,12,13,14] Advantages of this drug are easy availability, repeatability, economical pricing, minimal complications, and easy administration of the drug.[5,7,8] The drug has been routinely used in our set up since many years now in the usual IV mode of administration. The use of this drug is not limited to arthroplasty surgeries, but in other traumatic situation requiring quick hemostasis.[2,5] In fact, topical use of this drug is prevalent in many dental, cardiac, and spinal surgeries.[21,22,23] Wong et al., did the first trial on intraarticular administration of this drug and reported significant blood loss prevention using this mode.[2] But this trial did not have any inbuilt controls of IV TXA. They also evaluated the plasma level of this drug after topical administration and showed significantly less (70% less) levels as compared to an equivalent IV dose. The authors have concluded that there might be some action, albeit minimal due to systemic absorption of the drug. But these levels were taken more than 1 h after application of the drug. It has been proven that the action of TXA is actually only in the first few hours after surgery as it acts as a fibrinolytic inhibitor. This 1 h after tourniquet release is the crucial time when this drug achieves maximal hemostasis.[9,14] In fact, in our study we open the suction drain after an hour of application and still have managed excellent results, proving that this 1 h is the most important time for action of this drug. It has been shown that maximum plasma concentration is achieved in 30 min after intramuscular administration.[24,25] Also the half-life of the drug is less than 3 h,[2,3,10] and therefore there is rapid decrease in plasma levels of the drug. Therefore, the plasma values that Wong et al., have measured might be misleading. Ishida et al.,[6] Sa-Ngasoongsong et al.,[7] and Roy et al.,[8] have conducted similar studies recently, but both of them have used normal saline placebos. To actually prove the topical efficacy of this drug it has to be compared with an IV control group. This is what we have done in our study and as our results have shown better results for the intraarticular administration group it clearly proves that the drug has a good local action in curtailing postoperative blood loss.
In comparison with Wong et al.,[2] our study had a few differences in methodology and results. Firstly, as mentioned before, we are comparing intraarticular administration with IV administration and not placebos. Secondly, our method of administration was also a little different. They have applied the drug topically on the surface of the exposed wound before closure, without any drain and then release of tourniquet only after pressure bandaging. We instead practiced deflation of tourniquet at the end of cementation, careful hemostasis, and wound closure followed by drug delivery by injection. We believe this leads to better hemostasis and importantly identification of any inadvertent large vessel leak. We also routinely used a suction drain, but opened it only after 60 min which we felt were sufficient for the topical action of the drug. The same practice has been advocated by others like Sa-Ngasoongsong et al.[7] We used a lesser dose for intraarticular injection (1 g) as compared to their intraarticular administration (1.5 g). Since both studies calculated blood loss by means of difference in pre- and postop hemoglobin the timing of tourniquet should not be a confounding factor. We obtained slightly better results with this technique than Wong et al., in terms of total blood loss with intraarticular administration of 1.5 g TXA (1,020 mL as compared to 1,295 mL). In another subset where they used 3 g instead of 1.5 g of TXA, they got slightly lesser blood loss (1,208 mL), but still more than what we got in our study. On the other hand with the use of 3 g, they managed to reduce the amount of blood transfusion to zero. In our study the blood transfusion rate was similar to their 1.5 g (13%). Higher dose, even to the extent of more than 4 g, is an option which we have not studied, but surely looks promising. A yet to be published study by Maniar et al.,[10] have compared five regimens of TXA, which includes one local application method. They have shown local application to have good results as compared to single dose and intraoperative doses of TXA. But a three dose regimen gave better results than only local application. But a triple/double dose regimen compared with a single dose regimen of local application is not an identical study, which can be used to judge the efficacy of local application fairly.
In comparison with other trials on IV TXA for TKAs, we have found variable results in terms of blood loss control. We found significant reduction in decrease in hemoglobin. Blood transfusion rates and drain outputs were also less but not significant. Few trials have used total blood loss as their measure of blood loss and of them even fewer have used pre- and postop hemoglobin as the standard of this calculation. Even then the total blood loss for the intraarticular administration group in our study is less than most trials (1,020 as compared to 1,301 for Alvarez et al.,[5] and 1,225 for Molloy et al.,[18]). Even the drain output was less than most studies (260 mL as compared to 385 mL of Good et al.,[17] and 478 for Zhang et al.[19]). On the other hand, blood loss and drain output for the IV group were equivocal with these studies.[5] Blood transfusion rate is difficult to compare because of the nonstandard criteria used for transfusion. When compared to studies using the same criteria as we used, the requirement for the topical group (13%) was comparable to other studies (12% for Alvarez et al.,[5] and 13% for Veien et al.,[16]) and slightly higher for the IV group (17.5%). This might be because we chose a lower value of hemoglobin (10 mg/dL for females and 11 mg/dL for males) as exclusion criteria for our study.
Complications rate and postop function were similar for both groups in our study. They are also comparable to all other studies of TXA, which again show a similar rate to non-TXA studies.[3,5,13,14] Special emphasis was given to study any increased risk of thromboembolic phenomenon since this is the greatest theoretical risk of this drug. But like most other studies,[3,9,14] our study also confirms that TXA, even topically has no increased risks. Although our study showed similar results for both groups it is seems practical that if any increased risks of thromboembolism did exist with this drug it would certainly be lesser with intraarticular administration than IV administration.[2] More extensive trials might be needed to confirm this theory.
Thus, we conclude that intraarticular use of TXA is as effective if not better than its IV use to control postoperative blood loss in TKA. With its low systemic absorption, this route forms a good alternative to the traditional IV route. It may also be used as an adjunct, increasing the potency while keeping the safety in check. Certainly more studies of larger numbers would be needed to substantiate the use of this route of TXA administration.
We believe that because of the low systemic toxicity and equal efficacy intraarticular administration of TXA can be used for high risk patients alone, or as adjunct to IV administration in order to reduce the IV dose and complications.
Source of Support:
Nil
Conflict of Interest:
None declared.
REFERENCES
- The postoperative, blood- sparing efficacy of oral versus intravenous tranexamic acid after total knee replacement. Anesth Analg. 2004;99:1679-83.
- [CrossRef] [PubMed] [Google Scholar]
- Intraarticular administration of tranexamic acid reduces postoperative blood loss in total knee arthroplasty: A randomized, controlled trial. J Bone Joint Surg [Am] 2010:2503-13.:92-13.
- [Google Scholar]
- Tranexamic acid in total knee replacement: A systematic review and meta-analysis. J Bone Joint Surg Br. 2011;93:1577-85.
- [CrossRef] [PubMed] [Google Scholar]
- Tranexamic acid for control of blood loss in bilateral total knee replacement in a single stage. Indian J Orthop. 2011;45:148-52.
- [CrossRef] [PubMed] [Google Scholar]
- Tranexamic acid reduces blood transfusion in total knee arthroplasty even when a blood conservation program is applied. Transfusion. 2008;48:519-25.
- [CrossRef] [PubMed] [Google Scholar]
- Intra-articular injection of tranexamic acid reduces not only blood loss but also knee joint swelling after total knee arthroplasty. Int Orthop. 2011;35:1639-45.
- [CrossRef] [PubMed] [Google Scholar]
- Postoperative blood loss reduction in computer-assisted surgery total knee replacement by low dose intra-articular tranexamic acid injection together with 2-hour clamp drain: A prospective triple-blinded randomized controlled trial. Orthop Rev (Pavia). 2011;3:e12..
- [CrossRef] [Google Scholar]
- Efficacy of intra-articular tranexamic acid in blood loss reduction following primary unilateral total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2012;20:2494-501.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness and safety of tranexamic acid administration during total knee arthroplasty. Vox Sang. 2008;95:39-44.
- [CrossRef] [PubMed] [Google Scholar]
- Tranexamic acid reduces early post-operative blood loss after total knee arthroplasty: A prospective randomised controlled trial of 29 patients. Knee. 2006;13:106-10.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of aminocaproic, tranexamic acids in the control of bleeding during total knee replacement: A randomized clinical trial. Br J Anaesth. 2006;96:576-82.
- [CrossRef] [PubMed] [Google Scholar]
- Most effective regimen of tranexamic acid in knee arthroplasty: A prospective randomized controlled study in 240 patients. Clin Orthop Relat Res. 2012;470:2605-12. Epub 2012 Mar 15, 10.1007/s11999-012-2310-y
- [CrossRef] [PubMed] [Google Scholar]
- Tranexamic acid (Cyklokapron) reduces perioperative blood loss associated with total knee arthroplasty. Br J Anaesth. 1995;74:534-7.
- [CrossRef] [PubMed] [Google Scholar]
- Mini-subvastus approach for total knee arthroplasty in obese patients. Indian J Orthop. 2010;44:292-9.
- [CrossRef] [PubMed] [Google Scholar]
- Practice guidelines for perioperative blood transfusion and adjuvant therapies. Anesthesiology. 2006;105:198-208.
- [CrossRef] [PubMed] [Google Scholar]
- Tranexamic acid given intraoperatively reduces blood loss after total knee replacement: A randomized controlled study. Acta Anaesthesiol Scand. 2002;46:1206-11.
- [CrossRef] [PubMed] [Google Scholar]
- Tranexamic acid decreases external blood loss but not hidden blood loss in total knee replacement. Br J Anaesth. 2003;90:596-9.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of topical fibrin spray andtranexamic acid on blood loss after total knee replacement: A prospective, randomized controlled trial. J Bone Joint Surg [Br] 2007:306-9.:89-9.
- [CrossRef] [PubMed] [Google Scholar]
- A meta-analysis of tranexamic acid to reduce blood loss in total knee arthroplasty. Chinese J Orthop. 2009;29:524-9.
- [Google Scholar]
- Intraarticular administration of antifibrinolytic drugs for on-pump cardiac surgery: A systematic review and meta-analysis. Can J Anesth. 2009;56:202-12.
- [CrossRef] [PubMed] [Google Scholar]
- Can local application of Tranexamic acid reduce post-coronary bypass surgery blood loss? A randomizedcontrolled trial. J Cardiothoracic Surg. 2009;4:25..
- [CrossRef] [PubMed] [Google Scholar]
- Hemostatic effect of tranexamic acid mouthwash in anticoagulant-treated patients undergoing oral surgery. N Engl J Med. 1989;320:840-3.
- [CrossRef] [PubMed] [Google Scholar]
- Application of pharmacokinetics data from healthy volunteers for the prediction of plasma concentrations of tranexamic acid in surgical patients. Clin Drug Invest. 1995;10:280-7.
- [CrossRef] [Google Scholar]
- Absorption and excretion of tranexamic acid following intravenous, intramuscular and oral administrations in healthy volunteers. Jpn J Clin Pharmacol Therapeutics. 1976;7:375-82.
- [CrossRef] [Google Scholar]




